Hyperbaric Oxygen Therapy for Necrotising Soft-Tissue Infections
Necrotising fasciitis and related "flesh-eating" infections are rare, fast-moving and life-threatening. Hyperbaric oxygen is used alongside urgent surgery and antibiotics to help fight the infection.
What this means for you
What is a necrotising soft-tissue infection?
A necrotising soft-tissue infection is a severe infection that spreads quickly through the skin, fat and the tough layer beneath called the fascia. The best-known form is necrotising fasciitis, sometimes called a "flesh-eating" infection. It can destroy tissue within hours and make a person very ill, so it is always treated as an emergency.
What are the warning signs?
Early on there may be pain that seems far worse than the skin looks, rapidly spreading redness or swelling, fever, and a feeling of being severely unwell. These infections can deteriorate fast, which is why urgent hospital assessment is essential.
How can hyperbaric oxygen help?
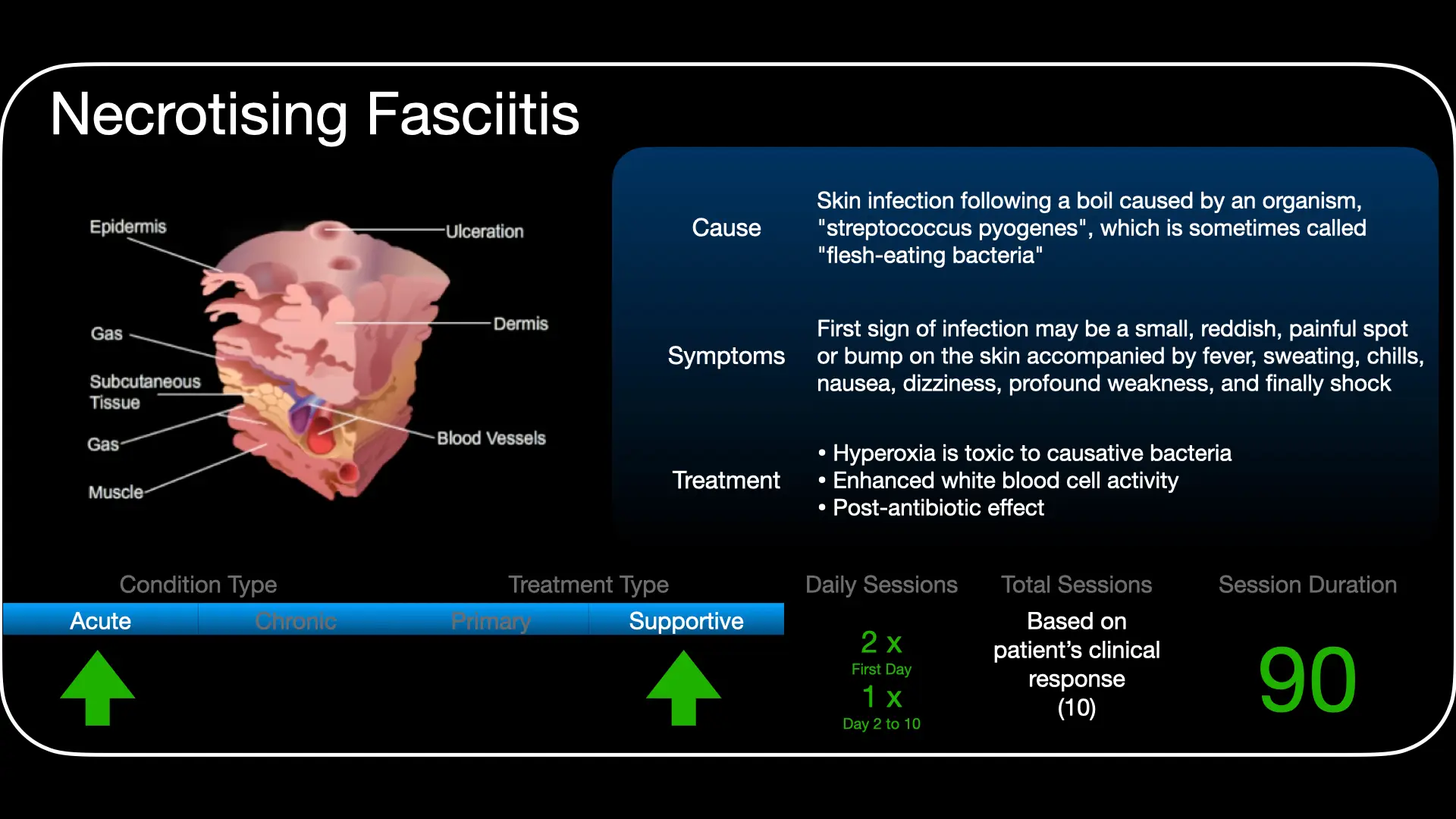
Hyperbaric oxygen is used together with surgery and antibiotics - not instead of them. Breathing pure oxygen under pressure drives a large amount of oxygen into the infected tissue. Many of the bacteria responsible struggle in an oxygen-rich environment, so this can help slow them, switch off some of their toxins, and support your body's own infection-fighting cells - helping to limit how far the infection spreads.
What to expect
When hyperbaric oxygen is used for this condition it is given urgently and often several times in the first day or two, coordinated around your operations and intensive-care treatment. The schedule is decided by the team for your situation.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 NSTIs - Fighting with Oxygen (English)
NSTIs - Fighting with Oxygen (English) Veg Teen Vleisvretende Infeksies (Afrikaans)
Veg Teen Vleisvretende Infeksies (Afrikaans) For Patients: NSTIs (UHMS 11)
For Patients: NSTIs (UHMS 11)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Necrotising soft-tissue infections (NSTIs) - including necrotising fasciitis, Fournier's gangrene and related entities - are a recognised indication for adjunctive hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO supports, and never delays or replaces, the essentials: emergent surgical debridement, broad-spectrum antibiotics and critical-care resuscitation.
Pathophysiology
NSTIs spread along fascial planes with thrombosis of perforating vessels, producing progressive ischaemia and tissue hypoxia that the visible skin changes underestimate. Causative organisms are often polymicrobial (Type I) or group A streptococcal/clostridial (Type II), with exotoxin-mediated tissue destruction and systemic toxaemia. The hypoxic, necrotic environment favours anaerobic and facultative organisms.
Why oxygen matters
Raising tissue oxygen tensions is directly inhibitory to anaerobes, restores oxygen-dependent neutrophil oxidative killing, and can suppress clostridial and streptococcal exotoxin production. HBO also supports the microcirculation at the ischaemic margin and aids demarcation of non-viable tissue. The intended effect is to blunt progression and support host defences while surgery and antibiotics control the source.
Role in management
- Source control is paramount: early and repeated debridement to viable tissue takes absolute priority.
- Broad-spectrum antibiotics (with antitoxin agents such as clindamycin) and full resuscitation run concurrently.
- HBO is integrated early and coordinated with theatre - it must never delay surgery.
Treatment approach
When used, HBO is delivered on 100% oxygen at pressures commonly in the 2.0-3.0 ATA range, with several treatments in the first 24-48 hours and continued sessions thereafter, individualised to the surgical course and clinical response. Exact pressures, durations and frequency are set case by case at the unit.
Evidence base
Because randomised trials are impractical in this emergency, the evidence is observational - but for NSTI it is substantial and mostly favourable. Two registered meta-analyses report lower mortality with adjunctive HBO - Hedetoft 2021 (48,744 patients; mortality odds ratio 0.44, 95% CI 0.33-0.58) and Huang 2023 (mortality risk ratio 0.52) - and national-database studies agree (Soh 2012, adjusted OR 0.49; a 2024 US National Inpatient Sample analysis, mortality under 2% vs 5.9%). The most recent prospective multicentre cohort (Scandinavia, 2025) reported 30-day mortality of 7% with HBO versus 43% without.
These findings are consistent in direction but must be read with care: all are observational and confounded by patient selection, a Cochrane review found no randomised trials, and a systematic review concluded the efficacy evidence is scarce - one two-hospital cohort was non-significant. Notably, the investigators reporting the largest survival signals themselves call for a randomised trial. HBO is therefore a recognised adjunct, integrated early within a combined surgical, antimicrobial and hyperbaric strategy.
Bottom line: HBO is an early adjunct to urgent surgical debridement and antibiotics. The observational evidence consistently associates it with lower mortality, but patient-selection effects mean this is an association, not proof - and surgery remains the primary, time-critical treatment that HBO must never delay.
Talks & chapter reviews
Recorded talks and chapter/outcome reviews on this indication:
 UHMS Indications, Ch. 11 — Necrotising Soft-Tissue Infections
UHMS Indications, Ch. 11 — Necrotising Soft-Tissue Infections HBOT: Clinical Outcomes of NSTIs
HBOT: Clinical Outcomes of NSTIs HBOT for Necrotising Fasciitis (overview)
HBOT for Necrotising Fasciitis (overview) HBOT for Gas Gangrene & Necrotising Fasciitis
HBOT for Gas Gangrene & Necrotising FasciitisKey references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Necrotizing Soft-Tissue Infections (Ch. 11).
- Levett D, Bennett MH, Millar I. Adjunctive hyperbaric oxygen for necrotizing fasciitis. Cochrane Database Syst Rev. 2015;(1):CD007937.
- Hedetoft M, Bennett MH, Hyldegaard O. Adjunctive hyperbaric oxygen treatment for necrotising soft-tissue infections: a systematic review and meta-analysis. Diving Hyperb Med. 2021;51(1):34-43.
- Huang C, Zhong Y, Yue C, He B, Li Y, Li J. The effect of hyperbaric oxygen therapy on the clinical outcomes of necrotizing soft tissue infections: a systematic review and meta-analysis. World J Emerg Surg. 2023;18(1):23.
- Faunø Thrane J, Ovesen T. Scarce evidence of efficacy of hyperbaric oxygen therapy in necrotizing soft tissue infection: a systematic review. Infect Dis (Lond). 2019;51(7):485-92.
- Soh CR, Pietrobon R, Freiberger JJ, et al. Hyperbaric oxygen therapy in necrotising soft tissue infections: a study of patients in the US Nationwide Inpatient Sample. Intensive Care Med. 2012;38(7):1143-51.
- Toppen W, Cho NY, Sareh S, et al. Contemporary national outcomes of hyperbaric oxygen therapy in necrotizing soft tissue infections. PLoS One. 2024;19(3):e0300738.
- Hyldegaard O, Nekludov M, Arnell P, et al. Use of hyperbaric oxygen in patients with necrotizing soft tissue infections: a Scandinavian multicenter, prospective, observational cohort. Infect Dis Ther. 2025;14:1715-38.
- Wilkinson D, Doolette D. Hyperbaric oxygen treatment and survival from necrotizing soft tissue infection. Arch Surg. 2004;139(12):1339-45.
The Great Deceiver: Unmasking the Biological Warfare of "Flesh-Eating" Infections
1. The reality behind the headlines: understanding NSTIs
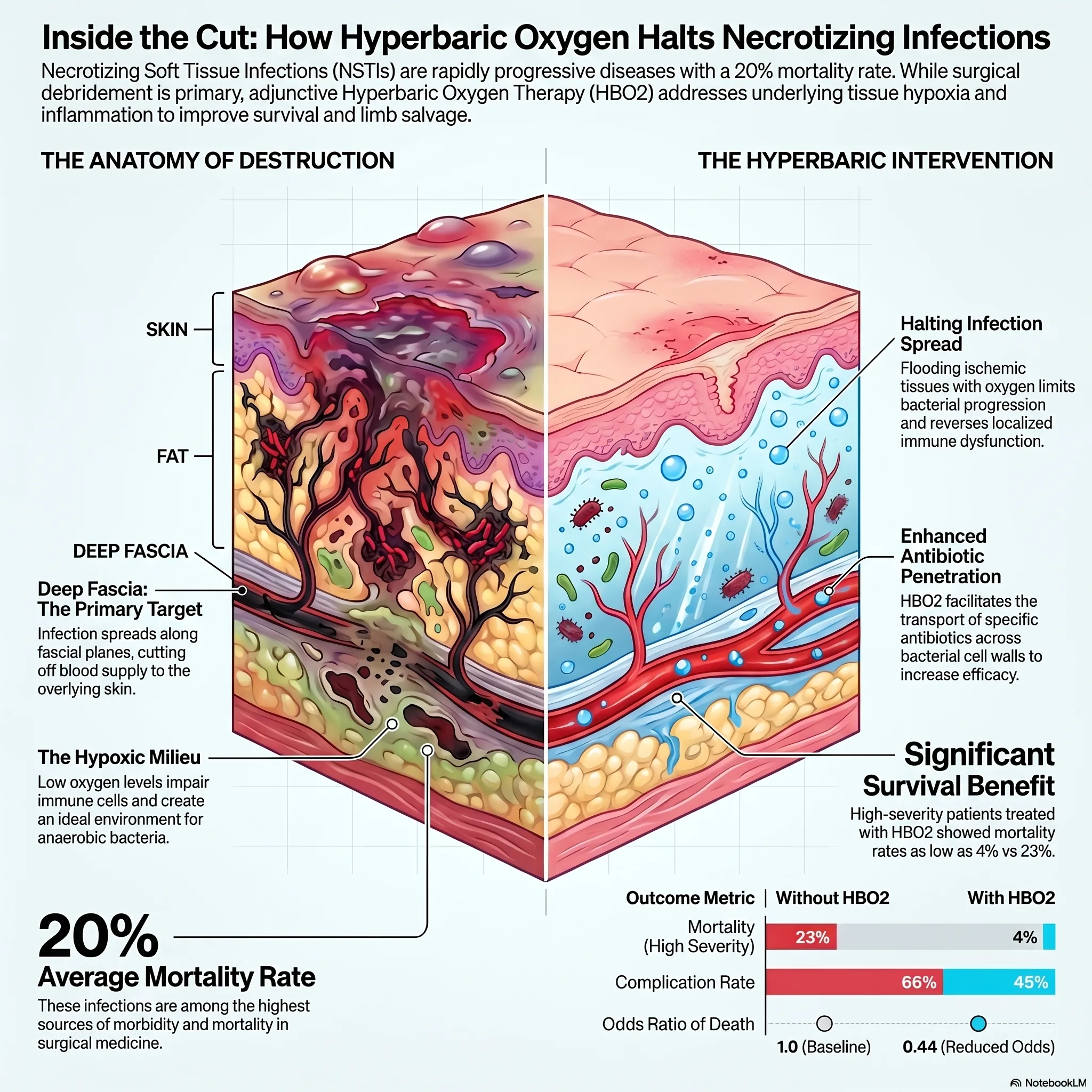
The term "flesh-eating bacteria" is a staple of sensationalist media, often used to conjure images of a terrifying, visible predator. In the clinical world, however, these conditions are known as Necrotising Soft Tissue Infections (NSTIs), and they are far more insidious than the headlines suggest. While the public focus remains on the dramatic "melting" of skin, the medical reality is a hidden, rapid, and often lethal destruction occurring beneath the surface. NSTIs are rare but aggressive clinical disorders that represent some of the highest sources of morbidity and mortality in modern medicine. In the United States, despite sophisticated intensive care, confirmed cases carry a staggering mortality rate of approximately 20%. Moving past the media narrative requires understanding that these are not just infections, but systemic biological emergencies.
2. The great deceiver: why "pain out of proportion" is the ultimate red flag
One of the most dangerous aspects of an NSTI is its ability to hide in plain sight. In the early stages, the skin over the affected area may appear relatively normal - perhaps slightly warm or swollen, easily mistaken for a common, non-lethal case of cellulitis. This is why clinicians call it the "great deceiver."
The infection's primary path of destruction is along the deep fascia, the connective tissue layers situated far beneath the skin and fat. Because the bacteria spread along these deep planes, the most critical early warning sign is "pain out of proportion" to the physical findings. A patient may be in agonising, unremitting pain while the surface of their limb shows only minor redness.
The physiological stakes are absolute: "time is tissue." The blood vessels that supply the overlying skin must pass through these deep fascial layers. As the infection progresses, it triggers oedema and necrosis within the fascia, strangling these vessels and cutting off the blood supply to the surface. When the skin finally turns dusky, grey, or black, it is a secondary sign that the underlying vasculature has already been destroyed. By the time the "flesh-eating" becomes visible, the war for the limb - or the life - is already at a critical tipping point.
3. Oxygen as a precision weapon: the science of hyperbaric therapy
While aggressive surgical debridement and broad-spectrum antibiotics are the traditional pillars of treatment, hyperbaric oxygen therapy (HBO2) has emerged as a powerful precision weapon. HBO2 is not merely "breathing air"; it is a sophisticated biological intervention that uses high-pressure oxygen to fundamentally alter the infection's environment.
Recent research, notably a 2021 observational study by Hedetoft and colleagues, has illuminated the "dual role" of this therapy. In what can be described as a "smart" intervention, HBO2 serves two distinct functions based on the patient's clinical state:
- Bacterial eradication: in stable patients, HBO2 creates an oxidatively stressed environment that facilitates bacterial death. It also acts as a force multiplier for antibiotics; for example, it enhances the penetration and post-antibiotic effect of aminoglycosides against notoriously difficult pathogens like Pseudomonas.
- Immune regulation: in patients suffering from septic shock, Hedetoft found that HBO2 can actually down-regulate the "cytokine storm" - the robust, self-destructive inflammation that leads to organ failure - by upregulating antioxidant defences like Heme Oxygenase-1 (HO-1).
By oxygenating ischaemic (oxygen-starved) areas, HBO2 essentially re-arms the body's natural "first responders" - the polymorphonuclear leukocytes - whose ability to kill bacteria is severely impaired in the low-oxygen environments created by these infections.
4. The 0.1% vs. 20%: how Group A Strep hijacks the immune system
"Type II" NSTIs, typically caused by Group A Streptococcus (GAS), present a unique "hidden complexity." Unlike Type I infections that target the elderly or those with underlying health issues, Type II often strikes younger, healthier individuals. Frequently, there is no "clear portal of entry", leading researchers to believe the bacteria may undergo haematogenous translocation - travelling through the bloodstream from a common site like the throat to the area of a minor, perhaps forgotten, injury.
The lethality of GAS is driven by its M proteins and superantigens. In a standard immune response, the body activates roughly 0.1% of its T-cells to combat a specific pathogen. However, streptococcal superantigens bypass the body's regulatory checks, triggering a catastrophic activation of up to 20% of the body's T-cells. This massive overreaction leads to "catastrophic shock", as the immune system's own defence mechanisms inadvertently cause widespread tissue destruction and rapid multi-organ failure.
5. The NSAID paradox: could common painkillers be a risk factor?
There is a growing and surprising body of evidence regarding the "NSAID paradox." While nonsteroidal anti-inflammatory drugs like ibuprofen are ubiquitous for managing pain, they may inadvertently hinder the body's ability to fight a burgeoning NSTI.
The concern is two-fold. Clinically, NSAIDs can mask the early symptoms - fever and pain - preventing a timely diagnosis of an infection that moves by the hour. Biologically, however, the impact is deeper. NSAIDs are reported to inhibit "monocyte superoxide production", effectively disarming the chemical weapons the immune system uses to kill bacteria. By interfering with neutrophil function and leukocyte adhesion, these common painkillers may inadvertently dampen the body's natural bactericidal control, allowing a virulent infection to accelerate unchecked.
6. Vulnerability in the smallest patients: the danger of omphalitis
The gravity of NSTIs spans the entire human lifespan, and perhaps nowhere is this more tragic than in neonates. In newborns, a seemingly routine infection of the umbilical cord stump - omphalitis - can escalate with terrifying speed into abdominal wall necrotising fasciitis.
The data for these smallest patients is sobering. A landmark report from Los Angeles Children's Hospital detailed a case series where 7 out of 8 neonates (87%) treated without HBO2 died. In these cases, a specific technical marker - violaceous discolouration of the skin - often signals the emergence of the necrotising process. Conversely, studies have shown that neonates who receive adjunctive hyperbaric treatment resolve systemic sepsis more rapidly and require fewer surgical debridements, significantly improving survival rates in a population that otherwise faces a grim prognosis.
7. Conclusion: a multi-front war against tissue death
Defeating necrotising soft tissue infections requires a multi-front war. It is a race against time that demands a multidisciplinary approach: aggressive surgery to remove necrotic tissue, precise antibiotic therapy to halt bacterial growth, and the physiological support of hyperbaric oxygen therapy to re-oxygenate dying tissue and modulate the immune response.
As we advance our understanding of these "great deceivers", we are left with a critical challenge in emergency medicine. While the survival benefits of HBO2 are increasingly clear - with some studies indicating it can reduce the odds of death by nearly 50% - access remains a significant hurdle. Many patients are far from hyperbaric facilities, and the logistics of transferring a critically ill, unstable patient can be daunting. We must ask ourselves how we can bridge this gap: if "time is tissue", the survival of the next patient may depend less on the virulence of the bacteria and more on our ability to ensure that advanced, life-saving therapies are available exactly when - and where - they are needed most.
This feature article is general educational information and does not replace advice from your own doctor or emergency services. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.