Hyperbaric Oxygen Therapy for Late Radiation Injury
Radiotherapy can leave tissue with a poor blood supply, causing problems months or years later - osteoradionecrosis, soft-tissue radionecrosis, radiation cystitis and proctitis. Hyperbaric oxygen helps by bringing new blood vessels and oxygen back to that tissue.
What this means for you
What is late radiation injury?
Radiotherapy is very effective against cancer, but over time it can also reduce the blood supply to the healthy tissue that was in the treatment field. Months or even years later, that tissue can become fragile and struggle to heal. Depending on where the radiation was given, this can show up as:
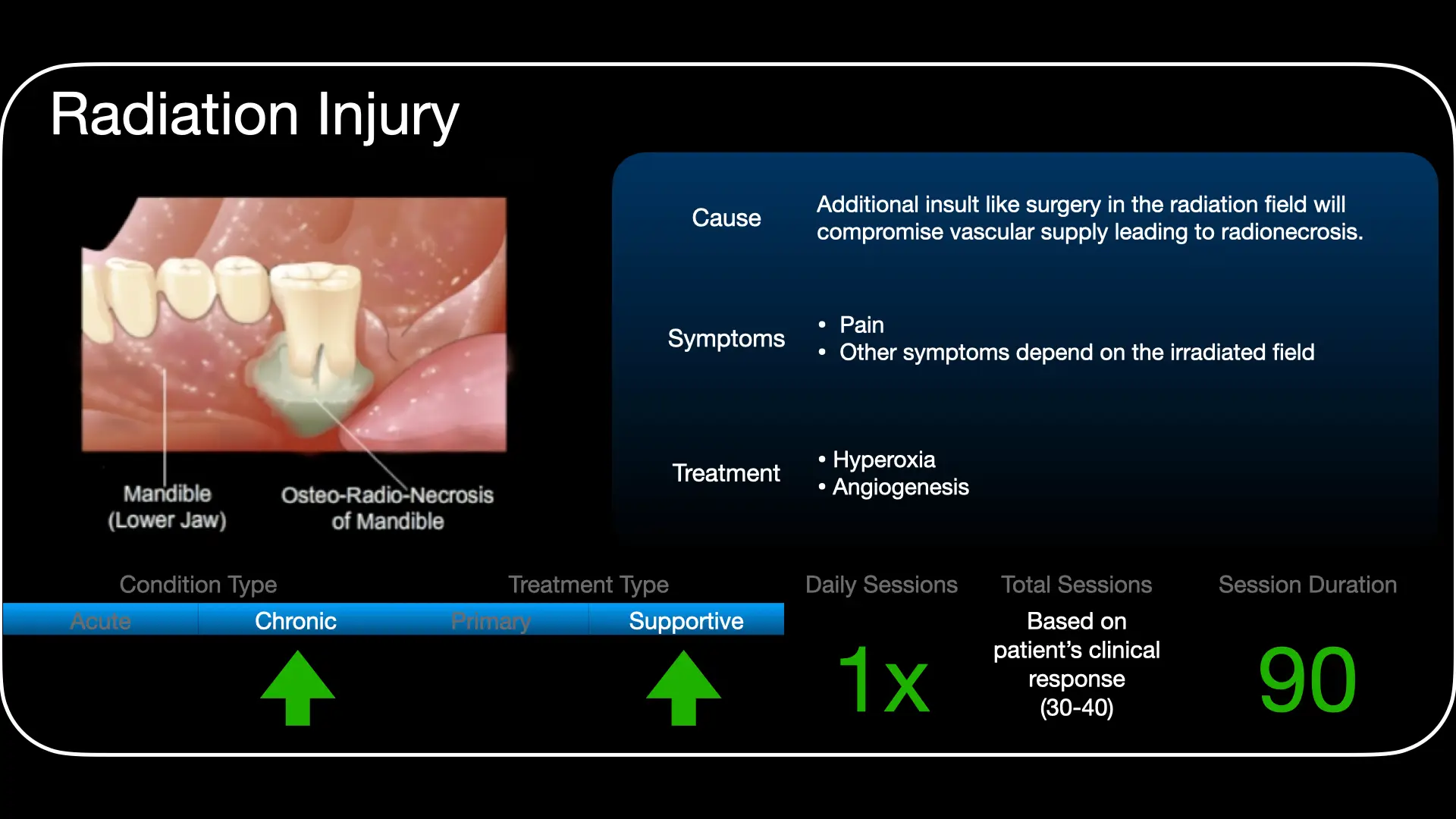
- Osteoradionecrosis - weakened, dying bone, most often in the jaw after head and neck radiotherapy.
- Soft-tissue radionecrosis - ulcers or wounds that will not heal, and stiff, fibrosed tissue.
- Radiation cystitis - a sore, bleeding bladder after pelvic radiotherapy.
- Radiation proctitis - a sore, bleeding lower bowel after pelvic radiotherapy.
How can hyperbaric oxygen help?
The core problem is that the tissue has too few blood vessels and too little oxygen. In the hyperbaric chamber you breathe pure oxygen under pressure, and - given as a course over several weeks - this gradually stimulates new blood vessels to grow into the damaged area and raises its oxygen level. That helps wounds heal, can reduce bleeding from the bladder or bowel, and supports surgery or dental work in a previously irradiated area.
What to expect
Treatment is usually a course of regular daily sessions over several weeks, with the number tailored to your problem and sometimes combined with surgery. Whether it is suitable depends on your history and the tissue involved.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Healing Radiation's Cost (English)
Healing Radiation's Cost (English) Straling: Skade & Genesing (Afrikaans)
Straling: Skade & Genesing (Afrikaans) For Patients: Late Radiation Injuries (UHMS 08)
For Patients: Late Radiation Injuries (UHMS 08)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Delayed (late) radiation tissue injury is one of the best-supported indications for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). It encompasses osteoradionecrosis (most commonly mandibular), soft-tissue radionecrosis, and haemorrhagic radiation cystitis and proctitis, as well as prophylaxis around surgery/dental extraction in irradiated fields.
Pathophysiology
Marx characterised late radiation injury as progressively hypoxic, hypocellular and hypovascular tissue (the "3-H" principle): endarteritis obliterans and fibrosis reduce capillary density and tissue oxygenation, leaving tissue unable to meet the demands of turnover, trauma or surgery, and prone to non-healing breakdown.
Why HBO works
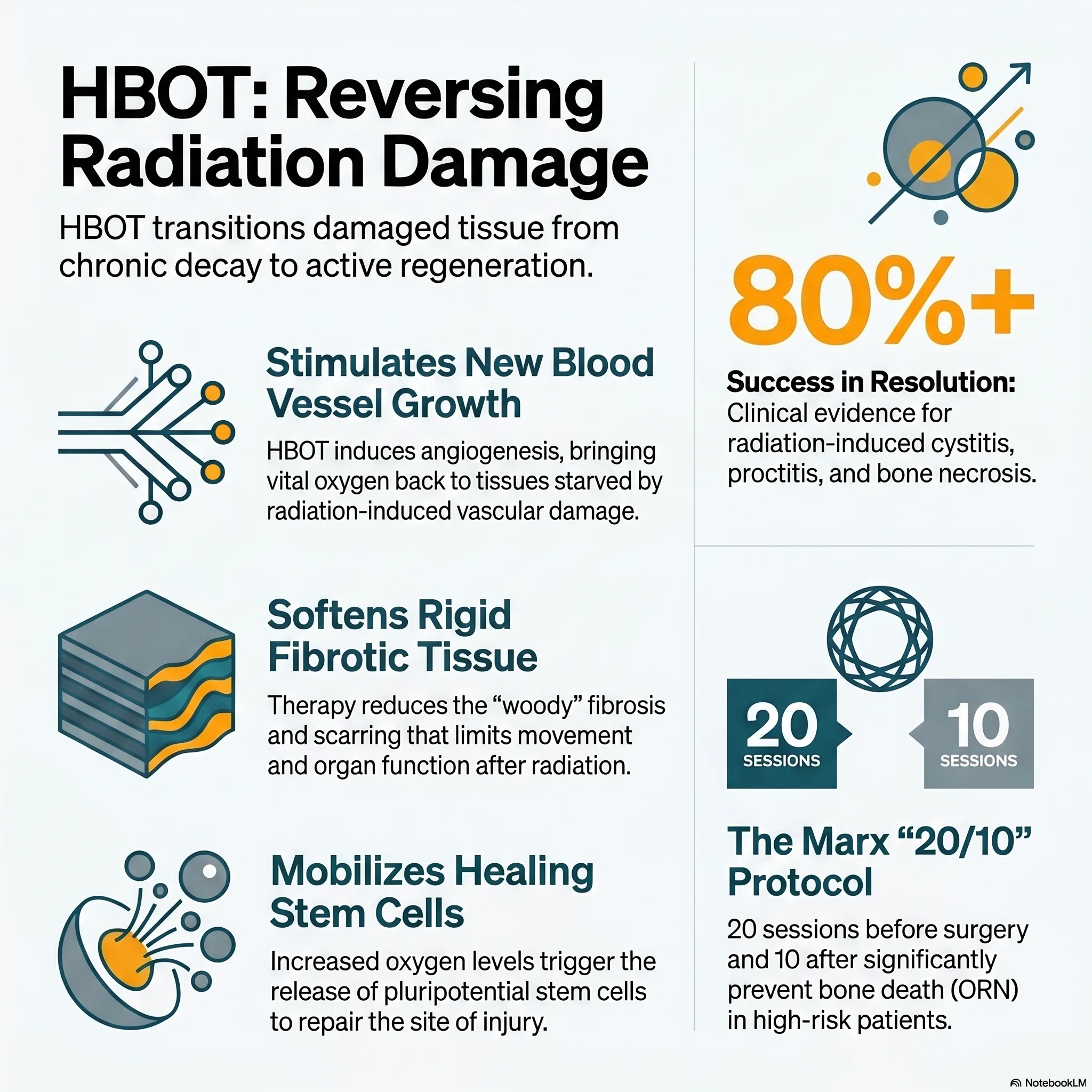
Intermittent hyperoxia establishes steep oxygen gradients that drive angiogenesis and neovascularisation, raising the capillary density of irradiated tissue toward a new, durable baseline. It supports fibroblast proliferation and collagen synthesis, mobilises stem/progenitor cells, and restores tissue oxygenation - reversing, in part, the hypovascular-hypoxic state. The gains in vascularity persist after a completed course.
Indications & role
- Osteoradionecrosis - combined with surgery per staged protocols (e.g. Marx); HBO alone for early/lower-stage disease.
- Soft-tissue radionecrosis and non-healing irradiated wounds; prophylaxis for extractions/surgery in irradiated bone.
- Haemorrhagic radiation cystitis and proctitis refractory to first-line measures.
Treatment approach
Courses are typically delivered on 100% oxygen at pressures around 2.0-2.4 ATA, daily, over roughly 20-40 sessions (with additional post-operative sessions where surgery is staged with HBO), individualised to the site and severity. Exact protocols are set case by case at the unit.
Evidence base
The evidence is strongest, and now most durable, for haemorrhagic radiation cystitis: the randomised RICH-ART trial (Oscarsson 2019) improved patient-reported urinary symptoms significantly over standard care, and 5-year follow-up (2025) showed the benefit was sustained. For osteoradionecrosis, HBO is best understood as an adjunct to surgery, not a standalone therapy - Marx's randomised prophylaxis data reduced post-extraction ORN from roughly 30% to 5%, and modern combined-trial data (Forner 2022) with a 2025 meta-analysis (HBO + surgery 69% vs HBO alone 38% vs surgery alone 36%) favour the combination.
We present the counter-evidence honestly. A double-blind RCT of HBO for established mandibular ORN (Annane/ORN96) was stopped early without benefit; a prophylaxis RCT (HOPON 2019) found no advantage where background ORN rates were low; a 2025 skull-base ORN meta-analysis found surgery far superior to conservative care (including HBO); the HOT2 trial (2016) found no benefit for chronic radiation bowel dysfunction (though Clarke 2008 was positive for proctitis); a breast late-toxicity RCT (HONEY 2024) missed its primary pain endpoint but reduced fibrosis; and randomised trials in brachial plexopathy and arm lymphoedema were negative. The consistent pattern is that soft tissue responds - cystitis, proctitis, and soft-tissue/mucosal fibrosis - while neural tissue and lymphoedema do not. A Cochrane review (Bennett 2016) concludes HBO improves outcomes in mandibular ORN, proctitis and cystitis, but not in neural tissue.
Bottom line
HBO is a selective adjunct for established, refractory late radiation injury of soft tissue and bone - strongest for haemorrhagic cystitis, and as an adjunct to surgery in osteoradionecrosis. It is delivered in coordination with oncology, surgical and dental teams, and is not a substitute for definitive surgical or urological care. Response depends on selection and on completing the course.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 08 — Delayed Radiation Injuries
UHMS Indications, Ch. 08 — Delayed Radiation Injuries HMP, Ch. 29 — Radiation Injury to Tissue
HMP, Ch. 29 — Radiation Injury to Tissue HBOT for Head & Neck Radiation Injury (ORN)
HBOT for Head & Neck Radiation Injury (ORN) HMP, Ch. 30 — Radiation Injury (Gynaecologic)
HMP, Ch. 30 — Radiation Injury (Gynaecologic) HBOT for Late Radiation Injury (overview)
HBOT for Late Radiation Injury (overview)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Delayed Radiation Injury (Soft-Tissue and Bony Necrosis).
- Marx RE. Osteoradionecrosis: a new concept of its pathophysiology. J Oral Maxillofac Surg. 1983;41(5):283-8. (Prophylaxis RCT: Marx RE, et al. J Am Dent Assoc. 1985;111(1):49-54.)
- Annane D, et al. Hyperbaric oxygen therapy for radionecrosis of the jaw: a randomized, placebo-controlled, double-blind trial (ORN96). J Clin Oncol. 2004;22(24):4893-900.
- Forner LE, et al. Hyperbaric oxygen treatment of mandibular osteoradionecrosis: combined data from DAHANCA-21 and NWHHT2009-1. Radiother Oncol. 2022;166:137-44.
- Geçkil N. Treatment approaches in cases of mandibular osteoradionecrosis: a systematic meta-analysis. J Stomatol Oral Maxillofac Surg. 2025;126(3):102316. doi:10.1016/j.jormas.2025.102316
- Shah SR, Wu A, Sindwani R, Tang D. Presentation and optimal management of anterior and central skull base osteoradionecrosis: systematic review and meta-analysis. Laryngoscope. 2025;135(3):982-90. doi:10.1002/lary.31817
- Oscarsson N, et al. Radiation-induced cystitis treated with hyperbaric oxygen therapy (RICH-ART): a randomised, controlled, phase 2-3 trial. Lancet Oncol. 2019;20(11):1602-14. (5-year follow-up: EClinicalMedicine. 2025.)
- Clarke RE, et al. Hyperbaric oxygen treatment of chronic refractory radiation proctitis: a randomised controlled trial. Int J Radiat Oncol Biol Phys. 2008;72(1):134-43.
- Glover M, et al. Hyperbaric oxygen for patients with chronic bowel dysfunction after pelvic radiotherapy (HOT2): a double-blind, sham-controlled RCT. Lancet Oncol. 2016;17(2):224-33.
- Mink van der Molen DR, et al. Hyperbaric oxygen therapy and late local toxic effects in patients with irradiated breast cancer (HONEY): a randomized clinical trial. JAMA Oncol. 2024;10(4):464-74. doi:10.1001/jamaoncol.2023.6776
- Bennett MH, et al. Hyperbaric oxygen therapy for late radiation tissue injury. Cochrane Database Syst Rev. 2016;(4):CD005005.
The Cellular Debt: Why Modern Cancer Precision is Failing Long-Term Tissue - and the High-Tech Oxygen Rescue
1. Introduction: the hidden aftermath of healing
For the modern cancer survivor, the final day of radiation often feels like a finish line. Yet, beneath the surface of apparently healthy tissue, a "hidden cellular debt" is often accruing. This period, known as the silent interval, can last for months or even decades while the patient feels entirely recovered.
Radiation is an undeniable lifesaver, but for 5% to 10% of patients, it leaves a "consequential effect" that traditional medicine is ill-equipped to handle. These late radiation tissue injuries (LRTI) are not merely side effects; they are deep biological failures. Hyperbaric oxygen therapy (HBO2) has emerged as the premier biological intervention capable of settling this debt and restarting the healing process.
2. The paradox of modern precision (IMRT)
It is a striking medical paradox: as our radiation technology has become more precise, the incidence of late-stage complications has not vanished. Innovations like intensity-modulated radiation treatment (IMRT) allow us to target tumours with sub-millimetre accuracy. This precision was expected to eliminate collateral damage, yet the rate of complications like osteoradionecrosis (ORN) remains stubbornly stable.
The reason for this paradox is a tactical trade-off known as dose escalation. Because IMRT is so effective at avoiding critical structures, oncologists have significantly increased the radiation doses delivered to the tumour to maximise cure rates. Essentially, we are winning the war on the tumour but losing the peace for the surrounding tissue.
Surgeons like Dr Robert Marx have observed that while tumours are better controlled, the tissues hit by these high-intensity "beamlets" suffer profound long-term damage. The surrounding healthy structures often receive higher intensity levels than they did in the era of less precise technology. We have traded acute survival for a complex, latent biological challenge.
3. More than just blood flow: the "fibroatrophic" model
For decades, the medical community viewed radiation injury as a simple plumbing problem - a lack of blood flow. Modern research has replaced this narrow view with the "fibroatrophic" model, which describes a far more sinister collapse of tissue infrastructure. In this model, the tissue isn't just starved of oxygen; it is being actively replaced by non-functional, "woody" fibrosis.
The primary culprit in this process is TGF-beta, the most frequently studied cytokine associated with radiation injury. This molecule drives the exuberant buildup of scarred collagen that robs organs of their elasticity. HBO2 intervenes by reducing this fibrosis and restoring "mechanical compliance", which is the critical ability of tissues to stretch and function.
"A combination of mechanical dilation and hyperbaric oxygen is recommended, employing a Marx-like '20 and 10' protocol of pre- and post-dilation HBO2."
4. The biological rescue team: stem cells and angiogenesis
HBO2 functions as a multi-stage biological rescue team that addresses the root causes of radiation-induced decay through three specific mechanisms:
- Angiogenesis: it stimulates the growth of entirely new capillary networks, permanently repairing the vascular "obliterative endarteritis" caused by radiation.
- Reduction of fibrosis: it actively breaks down the dense, scarred collagen mediated by TGF-beta, restoring the flexibility essential for organs like the bladder or larynx.
- Stem cell mobilisation: mediated by nitric oxide, HBO2 triggers the release of "pluripotential" stem cells from the bone marrow. These cells migrate to the site of injury and differentiate into the specific tissue types required to rebuild the damaged organ.
5. The surprising economics of oxygen
Beyond the humanistic victory of saving a patient's jaw or bladder, the financial data supporting HBO2 is overwhelming. Chronic radiation injuries are notoriously expensive to manage via traditional surgery, often requiring repeat procedures and intensive care stays. The elegance of hyperbaric prevention offers a clear alternative to the misery of repeat surgical failures.
The numbers tell a compelling story of fiscal responsibility. Integrated care for mandibular necrosis that utilises HBO2 costs approximately $96,000. In contrast, traditional surgical care without HBO2 support frequently soars to $226,000 due to high complication rates. Using prophylactic HBO2 before dental extractions is not just a clinical best practice; it is a profound win for the healthcare system's bottom line.
6. Debunking the great fear: does oxygen feed cancer?
A common physician concern is that a high-oxygen environment might "fuel" cancer growth or reactivate dormant tumours. This fear is intuitive, as HBO2 promotes the same vascular growth that tumours use to thrive. However, extensive clinical research has repeatedly addressed this concern with a resounding negative.
Comprehensive reviews by Feldmeier, Daruwalla, and Moen have synthesised decades of patient data to assess this risk. Their findings are unanimous: HBO2 does not enhance malignant growth or increase the rate of recurrence. In fact, some studies suggest that well-oxygenated tumours may actually be less aggressive and more responsive to treatment.
"Based on the present, as well as previous reviews, there is no evidence indicating that HBO2 either acts as a stimulator of tumor growth or as an enhancer of recurrence."
7. Conclusion: the future of quality of life
The goal of modern oncology is shifting from "survival at all costs" to the preservation of quality of life (QoL). New research, such as the "HONEY TRIAL", is currently investigating the potential for HBO2 to rescue breast cancer survivors from the pain and mobility issues of late radiation damage. We are also seeing promising results in treating xerostomia (dry mouth), where HBO2 helps restore salivary function.
The scale of the solution is already evident: delayed radiation injuries now account for approximately 40% of all hyperbaric medicine billings in the United States. With a resolution rate of 84% for conditions like radiation cystitis, the therapy is moving from the fringes to the centre of survivor care. As we successfully cure thousands of cancer patients today, we must ask: are we prepared to manage the latent injuries that will inevitably emerge in the survivors of tomorrow?
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.