Hyperbaric Oxygen Therapy for Compromised Grafts and Flaps
When a skin graft or flap is struggling because its oxygen supply is marginal, hyperbaric oxygen can support the at-risk tissue and improve its chance of survival.
What this means for you
What are grafts and flaps?
To close a wound or rebuild an area after injury or surgery, surgeons sometimes move healthy skin or tissue from one place to another. A thin layer of skin moved across is called a graft; a thicker piece moved with its own blood supply is called a flap. For either to survive, it must quickly get enough blood and oxygen in its new position.
What does "compromised" mean?
Sometimes a graft or flap does not get enough oxygen - the colour, temperature or healing look wrong, and it is at risk of partly or fully failing. This is called a compromised graft or flap. When this happens, hyperbaric oxygen can be used to help.
How can hyperbaric oxygen help?
In the chamber you breathe pure oxygen under pressure, which greatly increases the oxygen carried in your blood - including to tissue with a poor or marginal blood supply. This can support cells that are alive but struggling, encourage tiny new blood vessels to grow into the area, and improve the chance that the graft or flap takes and heals.
What to expect
Treatment is given as repeated daily sessions in the chamber, alongside the care of your surgical team, and continued while it is helping. Whether it is suitable depends on the type of graft or flap and your circumstances.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 HBO₂ for Grafts and Flaps (English)
HBO₂ for Grafts and Flaps (English) Asem Nuwe Lewe In (Afrikaans)
Asem Nuwe Lewe In (Afrikaans) For Patients: Grafts and Flaps (UHMS 05)
For Patients: Grafts and Flaps (UHMS 05)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
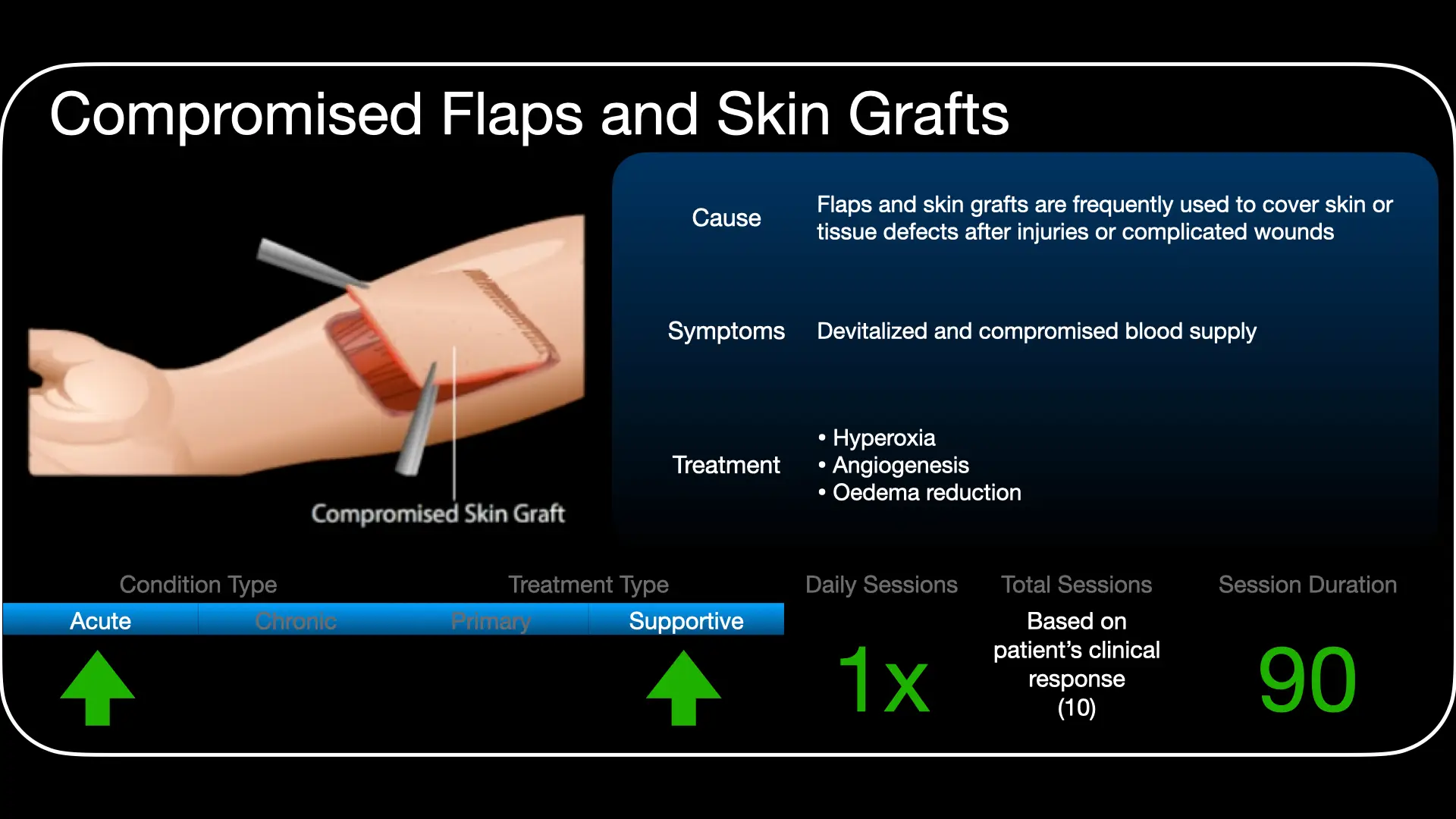
Compromised skin grafts and flaps are a recognised indication for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO is directed at grafts/flaps that are compromised or at risk from hypoxia or ischaemia - it is not indicated for routine, well-perfused, uncomplicated grafts.
Rationale
Graft and flap failure is driven by inadequate oxygen delivery to tissue whose perfusion is marginal, compounded by oedema, ischaemia-reperfusion injury and infection. The therapeutic window lies in tissue that is hypoxic but still viable; supporting it through the critical early period can be decisive for survival of the reconstruction.
Mechanisms
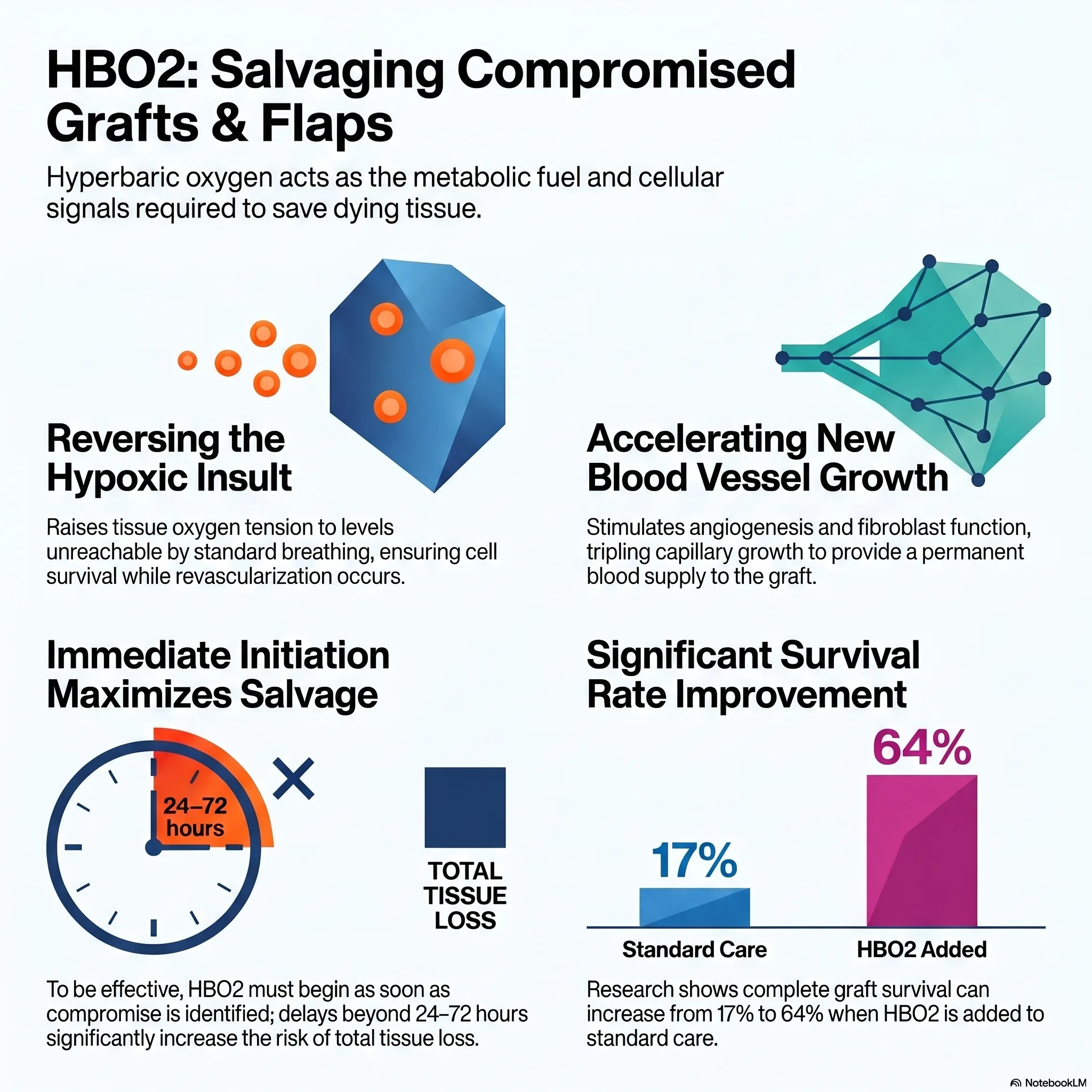
HBO sharply raises dissolved plasma oxygen and tissue oxygen tensions in hypoxic-but-viable tissue, supports cellular energetics, and reduces oedema through hyperoxic vasoconstriction without lowering oxygen delivery. It attenuates ischaemia-reperfusion and leukocyte-mediated injury, promotes fibroblast proliferation, collagen synthesis and angiogenesis/neovascularisation, and augments antibacterial defences - collectively improving graft take and flap survival.
Role in management
- Best results follow early initiation, as soon as compromise is recognised; delay reduces salvageable tissue.
- HBO complements - it does not replace - sound surgical technique, relief of mechanical/venous compromise, infection control and optimisation of perfusion.
- Patient selection is key: target marginal/at-risk tissue, not healthy grafts.
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.5 ATA, typically once or twice daily, continued while there is demonstrable benefit to the compromised tissue. Exact protocol and duration are individualised and set case by case at the unit.
Evidence base
The anchor is a randomised controlled trial (Perrins 1967) in compromised split-skin grafts: complete graft take 64% with HBO versus 17% without (number-needed-to-treat about 2). A modern randomised trial (Uniyal 2025) similarly found better graft uptake and faster donor-site healing in at-risk grafting, and two 2026 systematic reviews are positive - one (Carter 2026) issues a formal strong recommendation for peri-operative HBO, the other (He 2026) a large improvement in flap survival. HBO is a recognised UHMS indication (moderate-evidence tier) for grafts and flaps that are compromised or at risk.
We present the limits honestly. The Cochrane review (Eskes 2013) judged the overall trial base small and at risk of bias - "a lack of high-quality evidence" - and a controlled study (Vishwanath 2011) found no benefit from routine HBO on uncomplicated free flaps. So the evidence supports HBO for salvage of threatened tissue, not blanket cover of every graft or flap, and it is strongest when started early. (Note: the strongest recent review was produced with hyperbaric-society support, which we weigh accordingly.)
Bottom line
HBO is offered for grafts and flaps showing early signs of failure, and to prepare compromised (for example, previously irradiated) recipient beds before reconstruction. Started early, it can improve survival during the critical window before a durable blood supply forms. It is an adjunct to surgery - never a substitute for re-exploration when revision is needed - and it is not used routinely on healthy, well-perfused grafts or flaps.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 05 — Compromised Grafts and Flaps
UHMS Indications, Ch. 05 — Compromised Grafts and Flaps HMP, Ch. 28 — HBO in Skin Grafts and Flaps
HMP, Ch. 28 — HBO in Skin Grafts and Flaps HBOT for Compromised Grafts and Flaps (overview)
HBOT for Compromised Grafts and Flaps (overview)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Compromised Grafts and Flaps.
- Perrins DJD. Influence of hyperbaric oxygen on the survival of split skin grafts. Lancet. 1967;1(7495):868-71.
- Uniyal S, et al. The effect of hyperbaric oxygen therapy on split-thickness skin graft uptake in posttraumatic wounds and donor site healing: a randomized controlled trial. Wounds. 2025;37(3):134-40. doi:10.25270/wnds/24157
- Carter MJ, Eckert KA, Fife CE, Gelly HB. Systematic review of comparative studies evaluating hyperbaric oxygen therapy on skin flap and graft surgical indications. Plast Reconstr Surg Glob Open. 2026;14(5):e7750. doi:10.1097/GOX.0000000000007750
- He Z, Sun X, Chen J, Zhang M. Hyperbaric oxygen therapy for skin flap transplantation: a meta-analysis. J Wound Care. 2026;35(2):193-200. doi:10.12968/jowc.2023.0206
- Eskes A, Vermeulen H, Lucas C, Ubbink DT. Hyperbaric oxygen therapy for treating acute surgical and traumatic wounds. Cochrane Database Syst Rev. 2013;(12):CD008059. doi:10.1002/14651858.CD008059.pub3
- Francis A, Baynosa RC. Hyperbaric oxygen therapy for the compromised graft or flap. Adv Wound Care. 2017;6(1):23-32. doi:10.1089/wound.2016.0707
Under Pressure: 5 Surprising Ways Hyperbaric Oxygen Rescues Failing Reconstructive Surgeries
1. The hook: when perfection isn't enough
In the high-stakes theatre of reconstructive surgery, technical perfection is often the baseline, not the finish line. A surgeon can execute a flawless harvest and a meticulous microsurgical anastomosis, only to watch the tissue begin to succumb to a "nightmare scenario" in the recovery suite. The once-healthy pink of a skin flap may transform into the blue, turgid tint of venous congestion or the ashen, ghostly pallor of arterial ischaemia. When a graft or flap begins to fail due to factors beyond the reach of the scalpel - such as prior radiation, crushing trauma, or underlying hypoxia - the surgeon needs more than another suture. They need a specialised salvage technology.
Hyperbaric oxygen therapy (HBO2) is not a general wellness tool or a routine requirement for uncompromised, healthy surgeries. It is a targeted, Class IB intervention designed specifically for compromised tissue. By delivering 100% oxygen at pressures typically between 2.0 and 2.5 atmospheres absolute (ATA), HBO2 forces oxygen into solution in the plasma, providing a critical lifeline to tissues starved by ischaemia-reperfusion injury or metabolic demand.
2. The "vascular bridge": reimagining the recipient bed
The physiological survival of a reconstruction depends on how it interacts with its blood supply, and HBO2 acts as a bridge for the two primary reconstructive methods:
- Avascular grafts: these tissues are harvested without a dedicated blood supply and are entirely dependent on the "recipient wound bed" for oxygenation and revascularisation. HBO2 allows for larger grafts - such as the 2.0 cm composite grafts described in the Li et al. study - to thrive where they would normally exceed the bed's natural metabolic capacity.
- Inherent-supply flaps: these units include their own blood vessels but often face failure due to "random ischaemia" at the distal edges or microvascular collapse.
HBO2 serves as the ultimate safety net, keeping cells viable "while revascularisation takes place." By stimulating angiogenesis (the growth of new vessels) and enhancing fibroblast function, the therapy sustains the tissue during the precarious window before a functional blood supply is established. This prevents the devastating cycle of graft loss and the consequent donor-site morbidity - the high physical cost of harvesting from a new, healthy part of the body to fix a failed primary site.
3. Neutralising the "nicotine tax" on healing
Nicotine is a surgeon's adversary, acting as a potent vasoconstrictor that restricts blood flow and impairs microvasculature. While many surgeons delay or refuse elective procedures for active smokers, HBO2 offers a method to mitigate this "nicotine tax."
In pivotal animal models (Selcuk et al. and Demirtas et al.), nicotine exposure predictably decimated flap survival rates. However, the introduction of HBO2 neutralised this handicap, bringing survival rates in nicotine-exposed subjects back to parity with healthy controls.
Viable flap area improvement (Camargo et al.): tobacco-exposed control group, 47% viable area; tobacco-exposed + HBO2 group, 84% viable area.
By restoring survival rates to near-normal levels, HBO2 acts as a game-changer, allowing for the salvage of reconstructions in high-risk patients who would otherwise face near-certain necrosis.
4. The 24-hour "golden window"
In the world of surgical salvage, timing is the difference between a successful recovery and a total loss. "Expedient initiation" is the clinical mandate because the window for intervention is narrow. Once the microvasculature has completely collapsed, no amount of pressure can revive the tissue.
The Waterhouse et al. study provides a stark warning regarding the decline of success over time:
- Initiation within 24 hours: 89% complete salvage rate.
- Initiation between 1 to 3 days: only 25% salvage rate.
- Initiation after 3 days: 0% salvage rate.
This data emphasises that HBO2 must be viewed as an urgent response, not a last resort. When signs of flap compromise appear, every hour that passes brings the tissue closer to irreversible microvascular collapse.
5. The power of 1+1=3: multimodal salvage strategies
The most sophisticated outcomes are rarely achieved through oxygen alone; instead, they rely on a multimodal salvage strategy. When HBO2 is paired with other medical or biological agents, the synergistic effect can double the success rate of individual treatments.
- HBO2 + pentoxifylline: pentoxifylline is a rheologic agent that improves "erythrocyte flexibility", allowing red blood cells to deform and flow through narrowed capillaries. When combined with HBO2, research shows an 86% improvement over controls - a result nearly 40% more effective than using either therapy in isolation.
- HBO2 + medicinal leeching: for cases of total venous occlusion (where blood enters the flap but cannot exit), HBO2 alone is ineffective. However, when paired with medicinal leeches to mechanically drain the congestion, flap survival rates jump from 25% (leeching only) to 67%.
6. Saving the unsaveable: paediatric composite grafts
Perhaps the most impactful application of HBO2 is in the salvage of traumatic injuries in children, such as dog bites or ear amputations. These often require "large composite grafts" (>1.5 x 1.5 cm) that include skin, fat, and cartilage. Because children face a lifetime of potential secondary surgeries and emotional distress if a facial feature is lost, the "morbidity benefit" of HBO2 is immense.
A 2020 study by Camison et al. demonstrated that children with significant nasal or ear defects achieved a greater than 80% graft take when HBO2 was initiated immediately post-op. By saving the original tissue, surgeons avoid the "second wound" of additional harvesting and the complexities of prosthetic reconstruction.
Success snapshot: a 73-year-old female, who was a current smoker, underwent reconstruction for a basal cell carcinoma on the nasal dorsum. When the distal part of the advancement flap showed signs of necrosis, she began daily HBO2 at 2.0 ATA. After 20 sessions, she achieved complete resolution of the nasal tip necrosis, successfully salvaging a reconstruction that was actively failing.
Conclusion: the future of oxygen-led salvage
Hyperbaric oxygen therapy is firmly established as a Class IB intervention for compromised grafts and flaps. Its ability to inhibit ischaemia-reperfusion injury, stimulate neovascularity, and bolster fibroblast function makes it a cornerstone of modern reconstructive technology.
As we look toward the future of surgical planning, a fundamental question emerges: given the high financial and physical costs of a failed flap, should HBO2 be a "just in case" standby for every high-risk reconstruction? For the modern surgeon, the evidence suggests that the proactive application of oxygen under pressure is no longer just an adjunct - it is a vital tool for ensuring that technical perfection translates into clinical success.
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.