Hyperbaric Oxygen Therapy for Acute Thermal Burns
In serious burns, hyperbaric oxygen is used as an adjunct to standard burn care - to help reduce swelling, support injured-but-salvageable tissue, and aid healing.
What this means for you
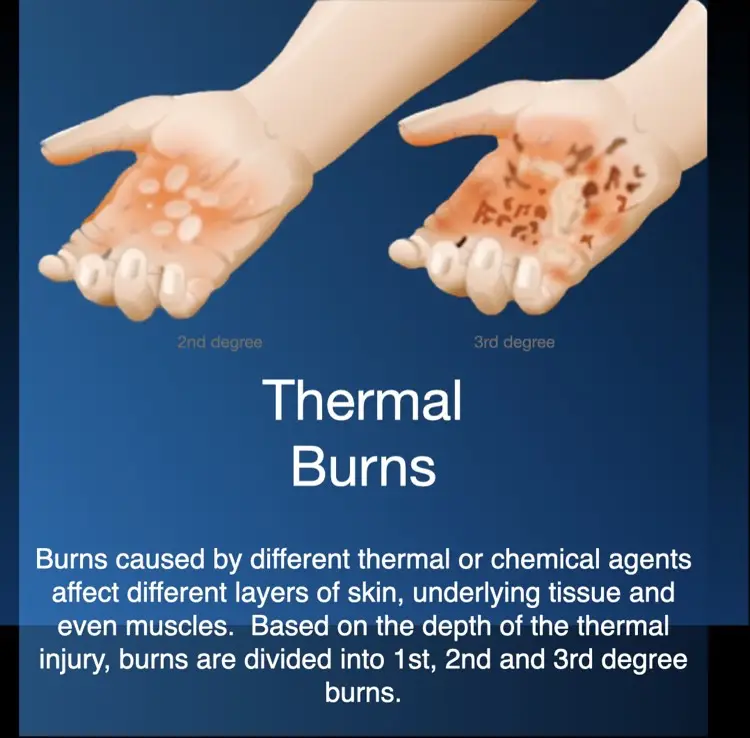
How burns injure tissue
A burn injures the skin and the tissue beneath it. Around the obviously destroyed area there is often a surrounding zone that is injured but not yet dead - sometimes called the "zone of stasis". In the hours and days after a burn, swelling and poor blood flow can tip that borderline tissue over into permanent damage, making the wound deeper and larger.
Where does hyperbaric oxygen fit in?
The foundation of burn treatment is specialist care: fluids, careful wound dressing, infection control and, when needed, surgery and skin grafting. Hyperbaric oxygen is used as an add-on in selected serious burns - never as a replacement for that care. By raising the oxygen reaching the injured area, it may help reduce swelling and support the borderline tissue so that less of it is lost.
What to expect
When hyperbaric oxygen is used for a burn it is started early and given as repeated sessions, carefully coordinated with the burns unit and fitted around dressing changes and any operations. Whether it is suitable depends on the size, depth and site of the burn and your overall condition.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Hyperbaric Oxygen for Burns (English)
Hyperbaric Oxygen for Burns (English) Veg Vuur met Lug (Afrikaans)
Veg Vuur met Lug (Afrikaans) For Patients: Thermal Burns (UHMS 14)
For Patients: Thermal Burns (UHMS 14) Thermal Burns — Explainer
Thermal Burns — ExplainerThis page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
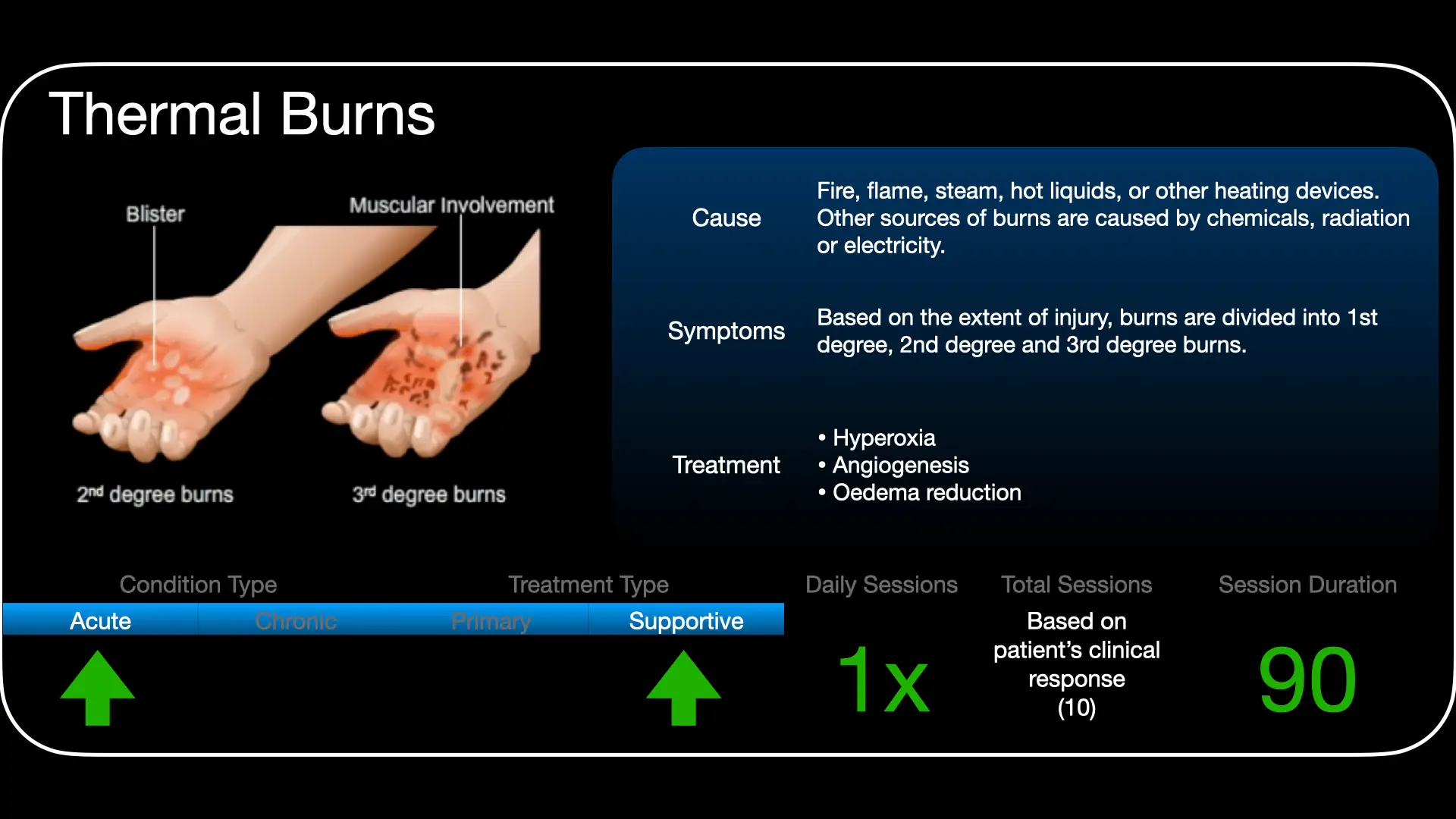
Serious thermal burns are listed among the indications for hyperbaric oxygen (HBO) therapy by the Undersea & Hyperbaric Medical Society (UHMS), where HBO is positioned as an adjunct to comprehensive burn care. It is not a substitute for resuscitation, wound management or surgery, and patient selection matters.
Rationale
The burn wound comprises Jackson's zones of coagulation, stasis and hyperaemia. The zone of stasis is potentially salvageable but vulnerable to progression from oedema, microvascular compromise, ischaemia-reperfusion injury and infection. The therapeutic aim of adjunctive HBO is to interrupt this secondary progression.
Proposed mechanisms
HBO markedly raises dissolved oxygen to ischaemic tissue, supports the zone of stasis, promotes vasoconstriction that reduces oedema without compromising oxygenation, preserves cellular energetics and the microcirculation, attenuates lipid peroxidation and leukocyte-mediated reperfusion injury, supports fibroblast function and angiogenesis, and augments antibacterial defences. The intended effect is reduced conversion of partial- to full-thickness injury and support of graft/wound healing.
Role in management
- HBO is integrated with - and never delays - fluid resuscitation, escharotomy/excision, grafting and infection control.
- Best considered early for selected deep partial-thickness or large burns; coordinated with the burns unit and intensive-care needs.
- Airway, ventilation and concurrent inhalational injury (including carbon monoxide) must be addressed and may themselves be indications for oxygen therapy.
Treatment approach
When used, HBO is delivered on 100% oxygen at pressures commonly in the 2.0-2.4 ATA range, started early and given as repeated daily sessions over the acute period; exact pressure, duration and frequency are individualised to the burn and the patient and set case by case at the unit.
Evidence base
The evidence for HBO in burns is genuinely mixed, and we present it that way. The biological rationale is strong - protecting the "zone of stasis", the ring of injured-but-salvageable tissue around a burn, so it does not deepen - and a large body of experimental and clinical reports is favourable. A 2024 review that pooled decades of studies found about two-thirds reported a positive result, and identified one clear practical lesson: lower chamber pressures (below 3 ATA) work better, which matches the pressures we use.
But the honest limitation is real: there is no large, well-designed randomised trial, the Cochrane review judged the evidence insufficient to confirm or refute benefit, and one small randomised pilot found no measurable effect. The professional bodies therefore rate this a moderate-evidence, adjunctive indication. HBO is offered selectively - for deeper burns over about 20% of the body, or burns of the hands, face, feet or perineum - started early, and always as an addition to full burn-unit care.
Bottom line
Added early (ideally within the first day) to specialist burn care, hyperbaric oxygen aims to preserve the salvageable tissue around a burn, reduce swelling and support healing and graft take. The rationale and most reports are favourable, but high-quality trial evidence is limited, so it is used selectively and with realistic expectations - never as a substitute for fluid resuscitation, surgery and burn-unit management.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 14 — Thermal Burns
UHMS Indications, Ch. 14 — Thermal Burns HMP, Ch. 31 — Adjunctive HBOT in Thermal Burns
HMP, Ch. 31 — Adjunctive HBOT in Thermal Burns Adjunctive HBO in Thermal Burns (talk)
Adjunctive HBO in Thermal Burns (talk) HBOT — Acute Thermal Burns (overview)
HBOT — Acute Thermal Burns (overview)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Thermal Burns.
- Smolle C, Auinger D, Lindenmann J, et al. Hyperbaric oxygen (HBO2) therapy in thermal burn injury revisited. Pressure does matter. A review. Undersea Hyperb Med. 2024;51(2):115-27. PMID 38985148.
- Cianci P, Slade JB Jr, Sato RM, Faulkner J. Adjunctive hyperbaric oxygen therapy in the treatment of thermal burns. Undersea Hyperb Med. 2013;40(1):89-108. PMID 23397872.
- Villanueva E, et al. Hyperbaric oxygen therapy for thermal burns. Cochrane Database Syst Rev. 2004;(3):CD004727. PMID 15266540.
- Chong SJ, Kan EM, Song C, et al. Characterization of early thermal burns and the effects of hyperbaric oxygen treatment: a pilot study. Diving Hyperb Med. 2013;43(3):157-61. PMID 24122191.
- Molina-Vega M, et al. Hyperbaric oxygen therapy for thermal burns: a systematic review. J Burn Care Res. 2026;47(3):917-22. doi:10.1093/jbcr/irag026
Why Hyperbaric Oxygen Could Be the 'Missing Link' in Modern Burn Care
For three decades, the clinical trajectory of severe burn recovery has remained stubbornly stagnant, hitting what researchers call the "survival floor." Despite relentless innovation in surgical grafting and specialised nutrition, patients with critical Baux scores between 70 and 110 face the same gruelling outcomes today that they did in the 1990s. We are left to wonder: is the missing link to breaking this plateau a technology we've had in our arsenal for sixty years?
Takeaway 1: stopping the "invisible" spread (the zone of stasis)
In 1965, Dr Wada observed a medical anomaly in Japanese coal miners treated for carbon monoxide poisoning: their concurrent burn injuries were healing with unprecedented speed. This discovery revealed that a burn is not a fixed event but a "three-dimensional" crisis that expands in both width and depth for up to 72 hours after the initial flame is extinguished. This period, known as the "zone of stasis", represents a precarious metabolic twilight where cells are failing but not yet dead.
HBO2 halts the "partial-to-full-thickness conversion" by preserving mitochondrial function and the ATP-driven sodium pump. By maintaining cellular energy production, clinicians can prevent the ballooning of endothelial cells and the "invisible" tissue death that would otherwise necessitate radical, life-altering surgery. This intervention essentially "buys time", allowing the surgeon to accurately define the injury rather than chasing a wound that is constantly growing.
"Burns are in this dynamic state of flux for up to 72 hours after injury... This progressive process may extend dramatically during the first early days after injury."
Takeaway 2: an 800% surge in healing potential (stem cell mobilisation)
Beyond merely keeping damaged cells alive, HBO2 acts as a systemic recruitment signal for the body's elite "repair crew." By stimulating bone marrow nitric oxide synthase, hyperbaric environments trigger a massive mobilisation of stem and progenitor cells into the bloodstream. HBO2 has been shown to increase marrow stem cell populations by a staggering 800%.
These mobilised cells migrate specifically to the site of the wound to function as de novo endothelial progenitor cells. This facilitates wound vasculogenesis - the biological creation of new blood vessels from scratch - rather than relying on the slow, traditional crawl of existing vessels into the damaged area. It is the difference between repairing a damaged road and paving an entirely new highway directly to a disaster zone.
Takeaway 3: slashing ventilator time in half (the inhalation injury breakthrough)
Smoke inhalation is the silent multiplier of mortality, increasing the death risk 24-fold for patients with otherwise manageable cutaneous burns. Traditionally, clinicians feared that high-pressure oxygen might exacerbate lung damage, but research by Ray and colleagues demonstrated the opposite. By dampening pulmonary inflammation and reversing the products of lipid peroxidation, HBO2 enables clinicians to wean patients off mechanical ventilation in a fraction of the usual time. This rapid recovery drastically reduces the window of vulnerability for secondary killers like pneumonia and sepsis.
| Treatment metric | With HBO2 | Without HBO2 |
|---|---|---|
| Days on ventilator | 5.3 days | 26 days |
| Total hospital days | 37 days | 76 days |
Takeaway 4: the economic paradox of burn care
The biology is sound, but the balance sheet is even more staggering. While the total cost for a survivor of a 60% TBSA burn averages over $1.4 million, a full course of adjunctive HBO2 treatments costs approximately $21,000. During the massive Taiwan theme park explosion disaster, HBO2-treated victims showed significantly higher graft survival and lower infection markers. This "economic lifeline" provides specific, inflation-adjusted savings of roughly $148,300 per case for inhalation injuries alone, by reducing:
- Surgical load: a 54% to 64% reduction in the need for debridement and skin grafting.
- Acute care duration: slashing weeks off the time spent in expensive ICU beds.
- Fluid efficiency: a 25% to 30% decrease in the massive fluid requirements needed to combat burn shock during initial resuscitation.
Takeaway 5: a new frontier in pain management
For a burn survivor, the trauma does not end when the fire is out; it continues through the agonising fog of neuropathic pain. Modern care often leans heavily on opioids, which carries a cruel irony: these narcotics suppress the very immune system the patient needs to survive. HBO2 offers a "central desensitisation" effect, helping the nervous system recalibrate its pain signals. This antinociceptive breakthrough is a form of clinical empathy, allowing the brain to "relearn" how to process signals without the debilitating fog of narcotics, ultimately protecting the patient's long-term psychological and immunological integrity.
Conclusion: the question that remains
After six decades of evidence - ranging from the serendipitous observations of coal miners to the rigorous data from the Taiwan explosion - the clinical case for HBO2 is compelling. Yet the therapy remains sidelined, often stymied by institutional inertia and a controversial 2009 Cochrane Review that many experts argue focused on the wrong metrics. Perhaps most telling was the 2016 Army Surgical Research Center study, which was poised to revolutionise military burn care before being abruptly cancelled without explanation.
As Dr J V Boykin noted, this therapy has the potential to provide a "much-needed elevation of the 'floor of survival'" for those who have lost everything to fire. We have the data, we have the technology, and we have the biological roadmap. If the evidence of HBO2's efficacy is so comprehensive, why are we still denying so many patients the benefit of this treatment?
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.