Hyperbaric Oxygen Therapy for Carbon Monoxide Poisoning
Carbon monoxide is a colourless, odourless gas - the "silent killer". Hyperbaric oxygen clears it from the blood far faster than ordinary oxygen and helps protect the brain from delayed injury.
What this means for you
What is carbon monoxide poisoning?
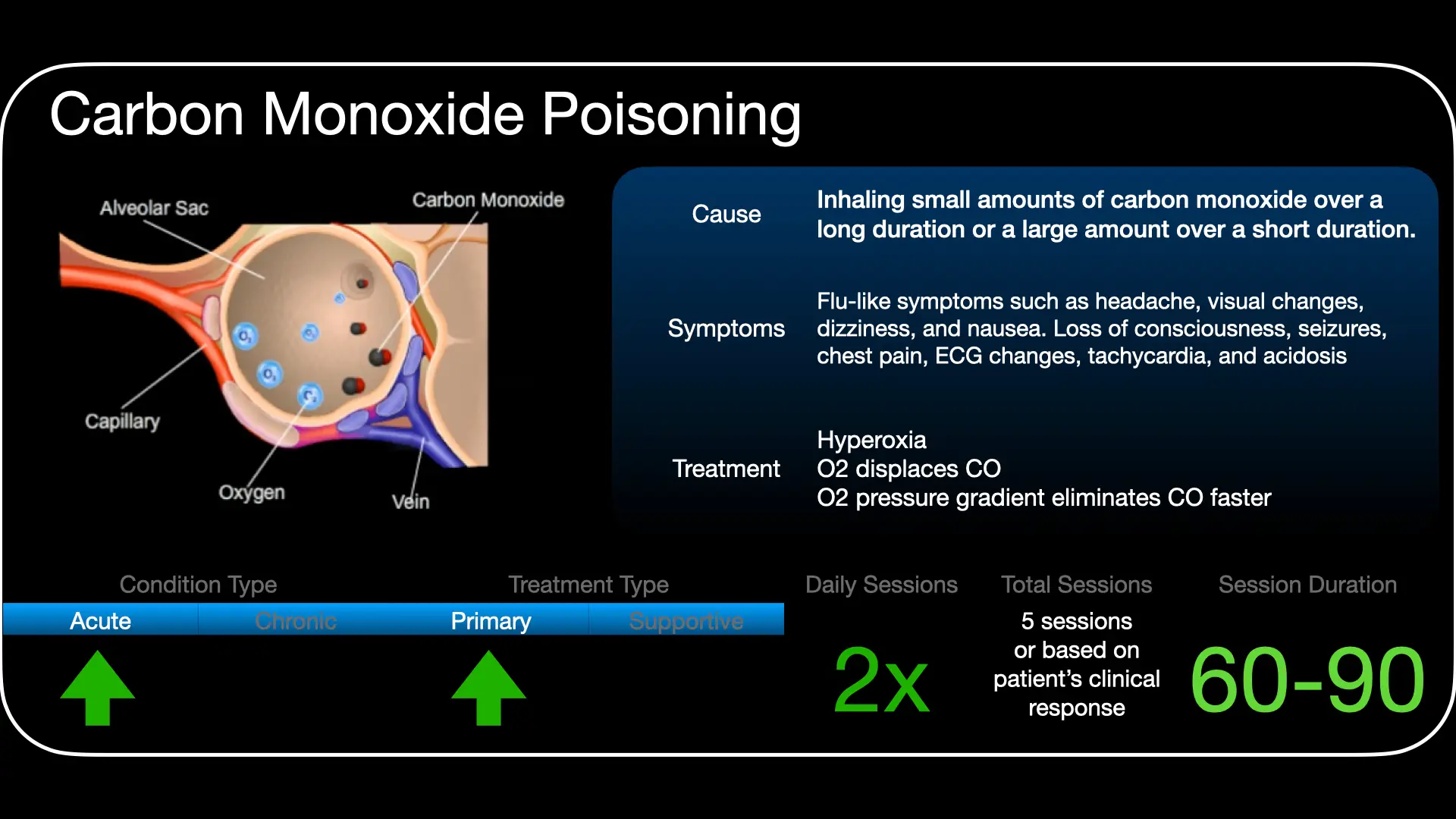
Carbon monoxide (CO) is a gas produced whenever fuel burns - from faulty heaters, gas appliances, generators, fires, or car exhaust in an enclosed space. You cannot see it, smell it or taste it. When you breathe it in, it sticks to the haemoglobin in your blood much more strongly than oxygen does, so your blood can no longer carry enough oxygen to your brain, heart and other organs.
What are the symptoms?
Early symptoms are easy to mistake for flu or food poisoning - headache, dizziness, nausea, tiredness and confusion. With higher exposure there may be breathlessness, chest pain, collapse or loss of consciousness. Because several people in the same building are often affected at once, a whole household feeling unwell together is an important warning sign.
How can hyperbaric oxygen help?
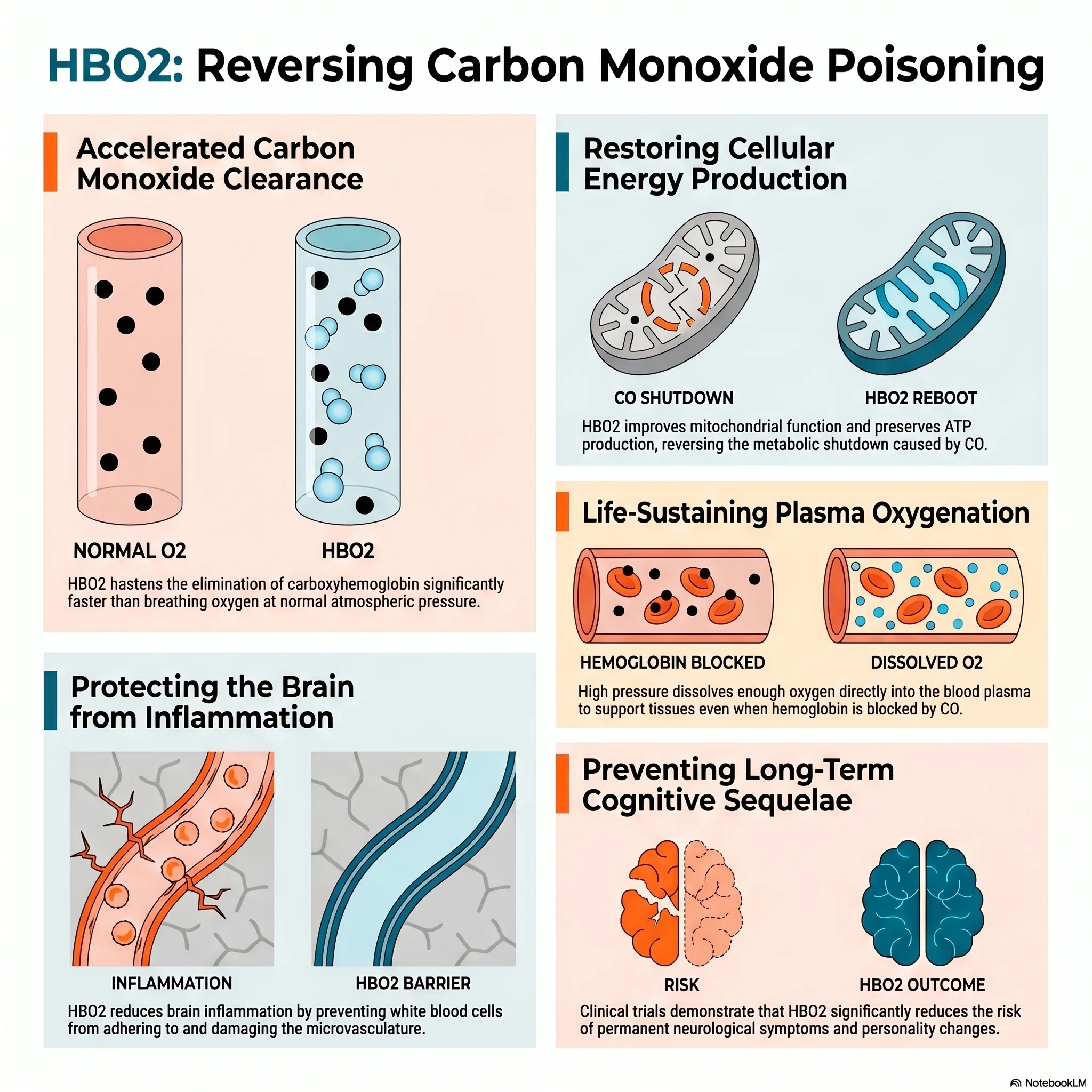
In the hyperbaric chamber you breathe 100% oxygen while the surrounding pressure is increased. This does two things: it clears the carbon monoxide out of your blood much faster than breathing ordinary air or even ordinary oxygen, and it dissolves a large amount of oxygen directly into your blood to supply organs that were starved. It is also used to help reduce the risk of the delayed brain and nerve problems that can sometimes follow serious CO poisoning.
Delayed effects to know about
Some people develop problems with memory, concentration, mood or movement in the days to weeks after the original exposure, even when they seemed to recover at first. These are called delayed neurological sequelae. Getting prompt, appropriate treatment is aimed at lowering this risk, and any new symptoms after a CO exposure should be reported to your doctor.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 The Silent Killer (English)
The Silent Killer (English) Die Stille Doder: Koolstofmonoksiedvergiftiging (Afrikaans)
Die Stille Doder: Koolstofmonoksiedvergiftiging (Afrikaans) For Patients: Carbon Monoxide Poisoning (UHMS 03)
For Patients: Carbon Monoxide Poisoning (UHMS 03) Carbon Monoxide Brain Damage
Carbon Monoxide Brain DamageThis page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Acute carbon monoxide (CO) poisoning is a long-established indication for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO is used to accelerate carboxyhaemoglobin (COHb) dissociation and, importantly, to reduce the incidence of delayed neurocognitive sequelae in selected patients.
Pathophysiology
CO binds haemoglobin with an affinity roughly 200-250 times that of oxygen, forming COHb and shifting the oxyhaemoglobin dissociation curve leftward - reducing both oxygen-carrying capacity and tissue offloading. Toxicity is not explained by hypoxaemia alone: CO binds cytochrome c oxidase and myoglobin, and drives a cascade of oxidative stress, lipid peroxidation, neutrophil activation and immune-mediated injury that underlies the delayed neurological syndrome.
Why pressure matters
The elimination half-life of COHb is roughly 4-6 hours on room air, around 60-90 minutes on 100% oxygen at 1 ATA, and approximately 20-30 minutes on 100% oxygen at ~2.5-3 ATA. Beyond faster COHb clearance, HBO restores mitochondrial cytochrome function, markedly raises dissolved plasma oxygen, and attenuates the leukocyte-mediated lipid peroxidation implicated in delayed injury.
Indications for referral & first aid
- Immediate high-flow 100% oxygen for all suspected cases; remove from the source.
- Consider HBO for: loss of consciousness, neurological signs or cognitive deficit, cardiac involvement (ischaemia/arrhythmia), pregnancy with significant exposure, or markedly elevated COHb (commonly cited thresholds around 25%, lower in pregnancy).
- COHb level confirms exposure but correlates poorly with severity; clinical features and the exposure history drive the decision. A normal pulse oximeter reading does not exclude poisoning (standard SpO₂ cannot distinguish COHb).
Treatment approach
Where HBO is indicated, treatment is given on 100% oxygen at pressures in the region of 2.4-3.0 ATA, ideally as early as possible after exposure; protocols and the number of sessions are individualised to severity and clinical response. Normobaric 100% oxygen is continued where HBO is not indicated or not immediately available.
Evidence base
The pivotal trial is the double-blind, sham-controlled RCT by Weaver (NEJM 2002): cognitive sequelae at six weeks occurred in 25% with HBO versus 46% with normobaric oxygen, a benefit sustained at 12 months. Two smaller randomised trials point the same way (Thom 1995; Ducasse 1995), and early treatment matters - a large matched cohort (Lee 2021) found significantly better outcomes when HBO started within about 6 hours. On this basis HBO is a recognised UHMS indication and is built into widely used clinical guidance.
We present the counter-evidence honestly, because it is substantial. Several randomised trials were negative (Raphael 1989 - no benefit without loss of consciousness; Scheinkestel 1999; Annane 2011), and the pooled meta-analyses are largely null: a Cochrane review found no significant benefit, a network meta-analysis (2022) found HBO no better than normobaric oxygen - and two sessions worse than one - and the newest guideline-linked review (2026) found no benefit even at higher pressures. The disagreement is largely methodological (control-group oxygen, protocol, timing). The practical read is to treat early and with a single or limited course, in appropriately selected patients.
Bottom line
HBO is offered for moderate-to-severe CO poisoning - loss of consciousness, neurological or cardiac signs, pregnancy, or high carboxyhaemoglobin - and is most likely to help when started within hours. The strongest single trial (Weaver) shows about a halving of cognitive sequelae, but the pooled trial evidence is mixed-to-null, and repeated sessions may do more harm than good. Emergency airway, cardiac and (in fire victims) cyanide treatment always come first and are never delayed for HBO.
Talks & chapter reviews
Recorded talks, textbook-chapter reviews and case discussions on this indication:
 UHMS Indications, Ch. 03 — Carbon Monoxide Poisoning
UHMS Indications, Ch. 03 — Carbon Monoxide Poisoning Hyperbaric Medicine Practice, Ch. 13 — Carbon Monoxide
Hyperbaric Medicine Practice, Ch. 13 — Carbon Monoxide Jain's Textbook, Ch. 13 — CO & Other Tissue Poisons
Jain's Textbook, Ch. 13 — CO & Other Tissue Poisons HBOT for Carbon Monoxide Poisoning (overview)
HBOT for Carbon Monoxide Poisoning (overview) HBOT for Carbon Monoxide Poisoning (overview 2)
HBOT for Carbon Monoxide Poisoning (overview 2) CO Mimics a Massive Stroke — case discussion
CO Mimics a Massive Stroke — case discussionKey references
- Weaver LK, Hopkins RO, Chan KJ, et al. Hyperbaric oxygen for acute carbon monoxide poisoning. N Engl J Med. 2002;347(14):1057-67.
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Carbon Monoxide Poisoning.
- Buckley NA, Juurlink DN, Isbister G, et al. Hyperbaric oxygen for carbon monoxide poisoning. Cochrane Database Syst Rev. 2011;(4):CD002041.
- Ho YW, Chung PY, Hou SK, et al. Should we use hyperbaric oxygen for carbon monoxide poisoning management? A network meta-analysis of randomized controlled trials. Healthcare (Basel). 2022;10(7):1311. doi:10.3390/healthcare10071311
- Fujita M, Todani M, Ajimi Y, et al. Evaluating the efficacy of hyperbaric oxygen therapy for acute carbon monoxide poisoning: a systematic review and meta-analysis. Acute Med Surg. 2026;13(1):e70114. doi:10.1002/ams2.70114
- Lee Y, Cha YS, Kim SH, Kim H. Effect of hyperbaric oxygen therapy initiation time in acute carbon monoxide poisoning. Crit Care Med. 2021;49(10):e910-e919. doi:10.1097/CCM.0000000000005112
The Invisible Saboteur: 5 Surprising Truths About Carbon Monoxide Poisoning
1. The silent threat in the room
Every year in the United States, an estimated 50,000 people are rushed to emergency departments due to carbon monoxide (CO) poisoning. We have been taught to view this gas as a simple "silent killer" that strikes through accidents or faulty furnaces, yet this narrative is dangerously incomplete. Despite decades of safety standards and the ubiquity of household alarms, CO remains one of the most misunderstood threats in modern medicine. To truly understand the risk, we must look past basic safety brochures and into the investigative reality: a complex systemic disease that can sabotage the human body long after the gas has cleared the room.
2. The blood test fallacy: overturning diagnostic dogma
For decades, the medical community has relied on the carboxyhaemoglobin (COHb) level - a measure of CO bound to red blood cells - as the gold standard for diagnosis. However, a growing body of clinical evidence is overturning this diagnostic dogma. We now know that COHb levels are a remarkably poor predictor of how sick a patient actually is or how much brain damage they have sustained.
A "low" level on a blood test often provides a false sense of security for clinicians and patients alike, but the source context is clear: "the COHb level is not predictive as a risk factor for CO-mediated morbidity or mortality." This is particularly terrifying in cases of "occult" or hidden poisoning, where low-level, chronic exposure can manifest as debilitating symptoms for weeks, months, or even years, often misdiagnosed while the underlying damage remains unaddressed.
3. The brain's inflammatory revolt: why the wiring fails
Most people assume CO kills by "suffocating" the cells - a simple lack of oxygen known as hypoxia. The investigative reality is far more sinister. CO triggers a biochemical cascade, an immunological revolt where the brain essentially turns on itself.
The damage is driven by the formation of adducts of myelin basic protein, which sparks a massive inflammatory response. This process is catalysed by the specific vulnerability of certain brain cells. As the research notes:
"In vitro cell cultures research demonstrates that oligodendrocytes are more susceptible to the toxic effects of CO than other brain cell types."
This is the "smoking gun" of CO-induced brain injury. Oligodendrocytes are the specialised cells responsible for producing myelin - the insulation for the brain's wiring. When CO attacks these cells, it creates a "biochemical cascade" that causes leukocyte (white blood cell) adhesion to the microvasculature. This means the injury is not a single event; it is an evolving inflammatory process that can worsen over weeks, leading to a permanent failure of the brain's internal communication system.
4. The ghost in the wall: the surprising physics of diffusion
There is a common, dangerous myth that carbon monoxide behaves like smoke, rising toward the ceiling or being trapped by standard walls. The physics of the gas suggests a much more porous world. While CO is technically 3% lighter than air, this difference is so negligible that its movement is governed not by buoyancy, but by diffusion.
Because CO behaves more like an expanding cloud than a rising plume, it "moves readily through drywall." This physical property has massive implications for public safety: you can be poisoned by a source you don't even own. Investigative data shows that residences without a single CO-producing appliance still require alarms because the gas travels from adjacent structures - such as a neighbour's attached garage where a vehicle was left running.
5. The decade-long debt: cardiac and neurological tolls
Survival is not the same as recovery. CO poisoning leaves a "long shadow" of delayed sequelae that can haunt a patient for a decade. This is not merely a "headache" that goes away; it is a systemic restructuring of health risks.
- Neurological decay: survivors face a high risk of dementia, cognitive decline, and a unique Parkinson's-like syndrome. Notably, this CO-induced parkinsonism has a distinct PET scan signature - specifically different from traditional Parkinson's disease - marking it as a unique pathological event.
- The 10-year cardiac debt: anyone who suffers initial cardiac injury during the poisoning event faces an increased risk of mortality for up to 10 years post-exposure. While standard echocardiography often provides "false reassurance", cardiac MRI (CMR) has emerged as the gold standard for identifying the hidden myocardial fibrosis CO leaves behind.
- Psychiatric shifts: there is a staggering incidence of "occult" symptoms including personality changes, depression, and anxiety that can persist for years after the physical traces of the gas are gone.
6. The molecular reset: why hyperbaric oxygen is non-negotiable
When treating CO poisoning, "fresh air" is not enough. Even 100% oxygen at normal pressure (normobaric) is often insufficient to stop the inflammatory cascade. To understand why, we must look at the half-life of the poison. On room air, it takes roughly 320 minutes to clear half the CO from the blood; on 100% oxygen, that drops to about 74 minutes.
However, hyperbaric oxygen (HBO2) therapy - breathing 100% oxygen in a pressurised chamber - does something standard oxygen cannot: it acts as a molecular medicine. HBO2 forces "dissociation", literally breaking the carbon monoxide away from the haemoglobin and cellular proteins (cytochromes) it has taken hostage. More importantly, HBO2 mechanistically inhibits leukocyte adhesion, effectively "shutting off" the inflammatory revolt before it can destroy the brain's myelin. It is not just about breathing; it is a molecular reset of the body's oxygen-processing machinery.
7. Conclusion: a public safety warning
The evidence is undeniable: carbon monoxide poisoning is not a one-time accident, but a complex, systemic disease. Our current safety infrastructure is failing to keep pace with this science. Current CO alarms are modelled on a 10% COHb level - a threshold that the source context explicitly warns may be "inadequate to protect populations vulnerable to damage", including pregnant women, children, and those with heart disease.
We must stop viewing CO safety as a matter of simple detection and start viewing it as a matter of aggressive clinical intervention. Until our alarm standards reflect the reality that even low-level exposure can trigger a decade of health complications, the "invisible saboteur" will continue to claim lives long after the sirens have stopped.
This feature article is general educational information and does not replace advice from your own doctor or emergency services. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.