Hyperbaric Oxygen Therapy for Air or Gas Embolism
A gas embolism is a bubble of gas trapped in the bloodstream. When it blocks an artery to the brain or heart it becomes a medical emergency - and recompression in a hyperbaric chamber is the definitive treatment.
What this means for you
What is an air or gas embolism?
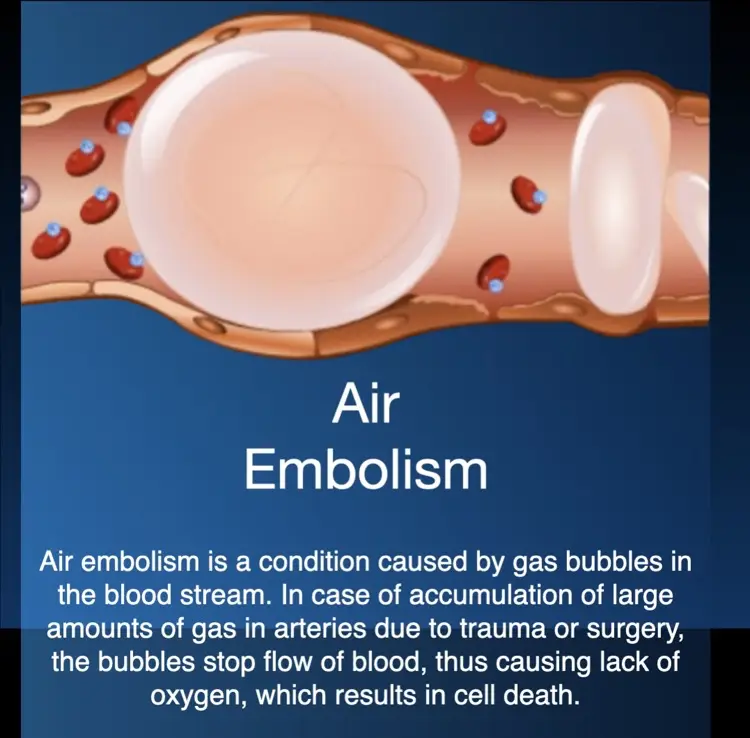
Your blood travels through arteries and veins as a continuous liquid. If a bubble of gas (most often air) gets into the bloodstream, it can be carried along until it reaches a vessel too narrow to pass - where it lodges and blocks the flow of blood, like an air-lock in a pipe. This blockage is called a gas embolism. When it blocks an artery to the brain or heart, the tissue beyond it is suddenly starved of oxygen, which can cause serious symptoms within seconds or minutes.
How does it happen?
Gas embolism can follow a scuba-diving injury (for example when a diver holds their breath while surfacing), but it can also happen during certain medical procedures - when a drip or central line is placed, during surgery, or during some keyhole operations. It is uncommon, but because it can be serious it is always treated urgently.
How can hyperbaric oxygen help?
Hyperbaric oxygen therapy is the definitive treatment for serious gas embolism, and it works in two ways. First, the chamber gently increases the pressure around you, which physically shrinks the gas bubble so blood can squeeze past it and circulation is restored. Second, breathing pure oxygen floods the affected tissue with oxygen and speeds up the natural disappearance of the bubble. Because pressure is involved, this is also called recompression therapy.
What to expect
Treatment is given as a session in the hyperbaric chamber, started as soon as possible, alongside the rest of your emergency care. The pressure, length and number of sessions are chosen for your situation. The earlier recompression begins, the better it tends to work.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Invisible Danger: Air Embolism (English)
Invisible Danger: Air Embolism (English) Die Borrel in die Bloed: Lugembolisme (Afrikaans)
Die Borrel in die Bloed: Lugembolisme (Afrikaans) For Patients: Air or Gas Embolism (UHMS 01)
For Patients: Air or Gas Embolism (UHMS 01)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
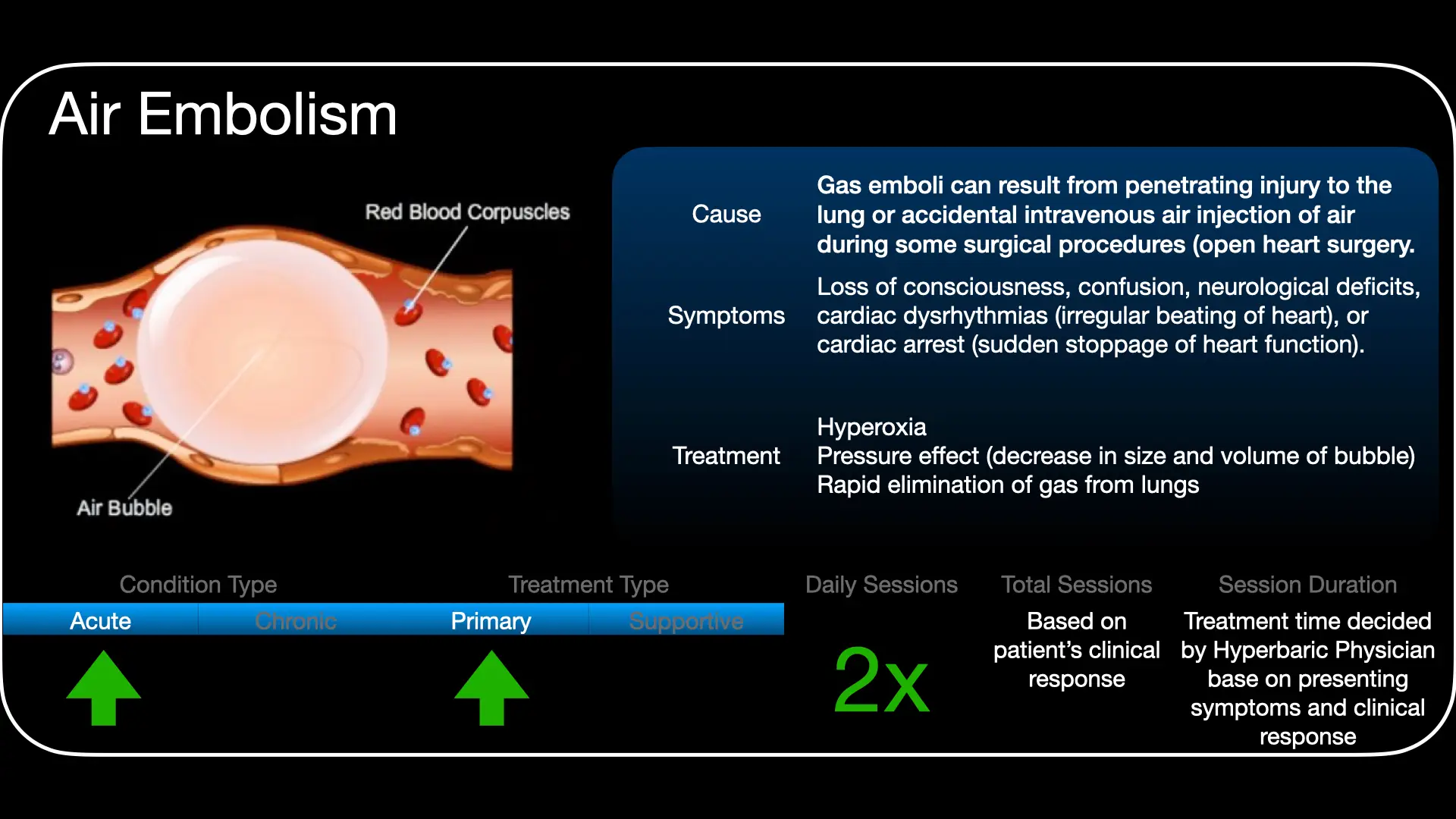
Arterial gas embolism (AGE) is among the first-listed and least controversial indications for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). Emergent recompression is the definitive treatment for clinically significant AGE, whatever the source - pulmonary barotrauma in divers, or iatrogenic air entry during vascular access, surgery, or endoscopic and laparoscopic procedures.
Pathophysiology
Gas enters the arterial circulation either directly (pulmonary barotrauma, a surgical field open to air) or by paradoxical/transpulmonary passage of venous gas. Intravascular bubbles obstruct flow, but injury is more than mechanical: bubble-endothelial contact triggers an inflammatory cascade, neutrophil adhesion and secondary thrombosis, which can produce progressive decline in cerebral blood flow and the well-described pattern of initial improvement followed by delayed deterioration.
Why recompression works
Two physical principles act together. By Boyle's law, raising ambient pressure reduces bubble volume (and diameter), restoring flow past the obstruction. Breathing 100% oxygen then maximises the inert-gas (nitrogen) washout gradient, accelerating bubble resolution, while raising dissolved plasma oxygen to oxygenate ischaemic tissue downstream. HBO additionally reduces post-ischaemic cerebral oedema and neutrophil-mediated reperfusion injury.
Immediate management & first aid
- Treat as a time-critical emergency - outcome correlates with the interval to recompression.
- High-flow 100% oxygen immediately; secure the airway and support circulation as needed.
- Keep the patient supine; avoid head-up positioning. Address the source (e.g. stop gas insufflation, clamp/aspirate a breached central line).
- Intravenous fluids; correct hypovolaemia. Arrange urgent transfer to the hyperbaric facility.
Recompression approach
Definitive treatment is recompression on 100% oxygen according to a recognised treatment table - most commonly a US Navy Treatment Table 6 (initial treatment depth equivalent to 2.8 ATA), with deeper initial compression and table extensions reserved for selected cases. The table, depth and number of follow-up sessions are individualised to the clinical response. Even when presentation is delayed, recompression is still indicated, as residual ischaemic and inflammatory injury can respond.
Evidence base
The rationale rests on sound physical principles, extensive animal data and a large body of clinical experience; AGE remains a recognised UHMS indication for which HBO is considered standard of care. A randomised trial of recompression versus no treatment is neither ethical nor feasible given the emergency nature of the condition, so the best evidence is observational - but it is consistent and, increasingly, quantified.
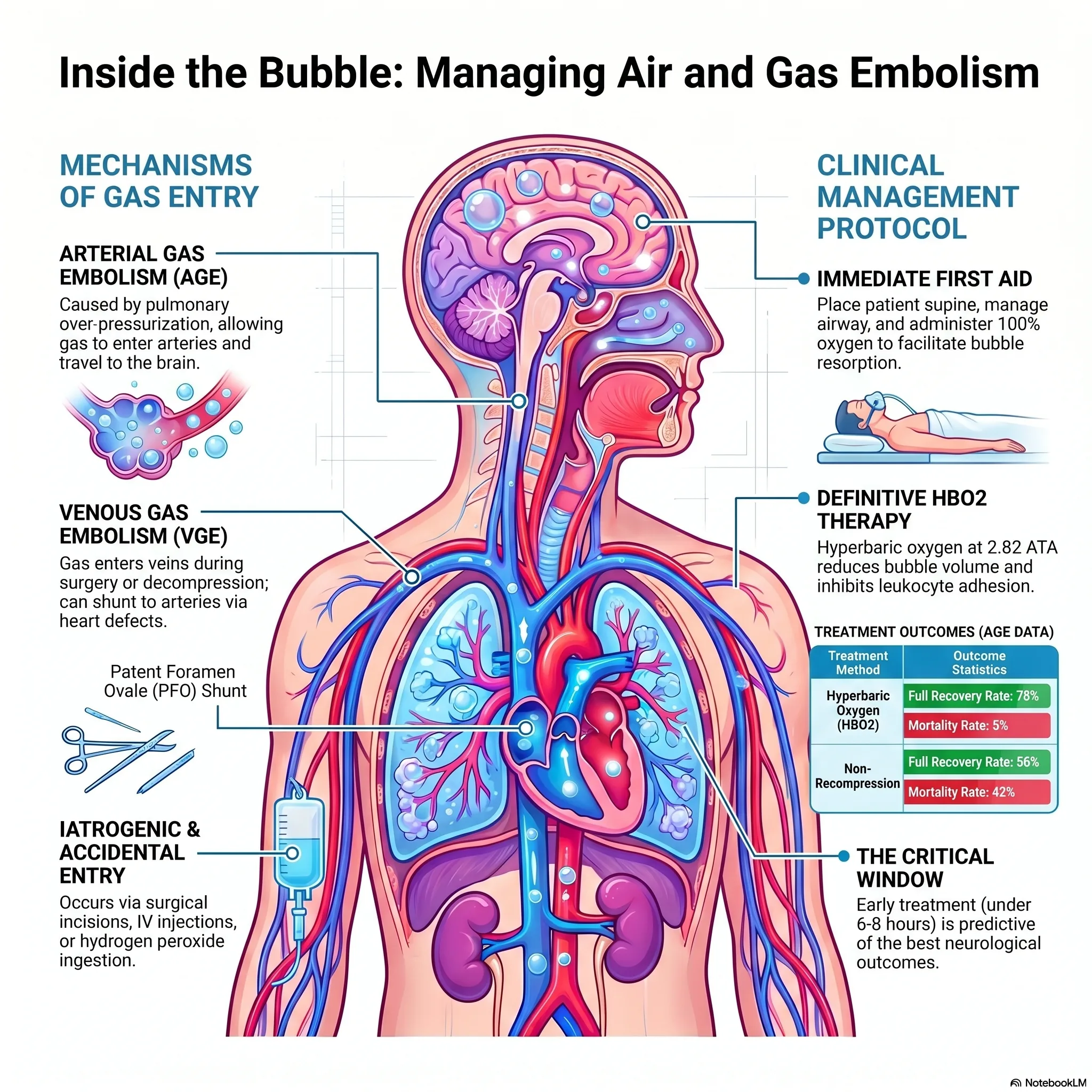
The strongest synthesis is an individual-patient-data meta-analysis of iatrogenic cerebral arterial gas embolism (Fakkert et al, 2023): the sooner recompression is started, the better the outcome, with the probability of a favourable recovery falling from roughly 65% when HBO is immediate to about 30% when it is delayed by around 15 hours. A prospective cohort from the same group (Fakkert et al, 2025) and the largest prospective inception cohort (Bessereau et al, 2010; 125 patients) both document substantial recoverable morbidity and confirm that delay to treatment predicts worse outcome, while a systematic review of 264 case reports (Hatling et al, 2019) shows HBO is the predominant specific treatment in practice.
Bottom line: none of these is a controlled trial of HBO versus no treatment, so they establish standard of care and the early-treatment imperative rather than trial-level proof of efficacy. Read together, they make a clear, evidence-based case for treating AGE as a time-critical emergency and beginning recompression as soon as possible.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 01 — Air or Gas Embolism
UHMS Indications, Ch. 01 — Air or Gas Embolism Hyperbaric Medicine Practice, Ch. 15 — Gas Embolism
Hyperbaric Medicine Practice, Ch. 15 — Gas Embolism Jain's Textbook, Ch. 12 — Cerebral Air Embolism
Jain's Textbook, Ch. 12 — Cerebral Air Embolism HBOT for Air or Gas Embolism (overview)
HBOT for Air or Gas Embolism (overview) HBOT for Decompression Sickness & Arterial Gas Embolism
HBOT for Decompression Sickness & Arterial Gas EmbolismKey references
- Moon RE, Mitchell SJ. Hyperbaric treatment of air or gas embolism: current recommendations. Undersea Hyperb Med. 2025;52(1):41-53.
- Moon RE (ed). Hyperbaric Oxygen Therapy Indications - Arterial Gas Embolism. Undersea & Hyperbaric Medical Society, 15th ed (2023).
- Mitchell SJ, Bennett MH, Moon RE. Decompression sickness and arterial gas embolism. N Engl J Med. 2022;386(13):1254-64.
- Fakkert RA, Karlas N, Schober P, et al. Early hyperbaric oxygen therapy is associated with favorable outcome in patients with iatrogenic cerebral arterial gas embolism: systematic review and individual patient data meta-analysis of observational studies. Crit Care. 2023;27(1):282.
- Fakkert RA, van Beers L, Weber NC, et al. Functional outcome and quality of life after iatrogenic cerebral air embolism treated with hyperbaric oxygen: a prospective cohort study. Diving Hyperb Med. 2025;55(4):330-37.
- Bessereau J, Genotelle N, Chabbaut C, et al. Long-term outcome of iatrogenic gas embolism. Intensive Care Med. 2010;36(7):1180-87.
- Hatling D, Høgset A, Guttormsen AB, Müller B. Iatrogenic cerebral gas embolism - a systematic review of case reports. Acta Anaesthesiol Scand. 2019;63(2):154-60.
- US Navy Diving Manual - Recompression Treatment Tables (Treatment Table 6).
- Vann RD, Butler FK, Mitchell SJ, Moon RE. Decompression illness. Lancet. 2011;377:153-64.
Bubbles in the Blood: 5 Surprising Truths About the World's Most Elusive Medical Emergency
The human circulatory system is traditionally viewed as a closed, pressurised loop of liquid life. However, this system is vulnerable to an invisible, often "stealth" intruder: gas. Whether it enters through a rupture in the pulmonary lining or via an iatrogenic accident during a routine medical procedure, a gas embolism - the presence of bubbles in the bloodstream - is a high-stakes emergency that can strike with devastating speed.
There are two primary classifications of this condition, defined by how the gas enters the vasculature. Arterial Gas Embolism (AGE) typically results from alveolar-capillary disruption, often triggered by pulmonary over-pressurisation (such as a diver holding their breath during ascent). Venous Gas Embolism (VGE) involves bubble formation in the veins due to decompression or the accidental injection of gas during surgery. While the body often filters small amounts of VGE through the pulmonary capillaries, the danger lies in the "stealth" conversion of VGE into AGE. This occurs when the pulmonary capillary network is overwhelmed or when gas crosses a right-to-left shunt, such as a patent foramen ovale (PFO), allowing bubbles to enter the cerebral circulation and manifest as a stroke.
Because this condition is frequently mischaracterised as a rare injury exclusive to the "abyss" of deep-sea diving, its most critical clinical truths are often overlooked. Here are five evidence-based realities of gas embolisms.
1. You don't have to be deep to be in danger
It is a common clinical misconception that gas embolisms require extreme depths. In reality, pulmonary barotrauma and the resulting AGE can occur in remarkably shallow water. Evidence indicates that a breath-hold ascent from as little as 1 to 2 metres - and in documented cases, a mere 0.75 metres - can trigger a life-threatening event.
This is biologically counter-intuitive but physically sound: the most significant proportional changes in gas volume occur nearest to the surface. Furthermore, some individuals are at risk even during "normal" ascents if they possess underlying pulmonary issues that trap air.
"AGE has been attributed to normal ascent in divers with lung pathology such as bullous disease and asthma."
2. The "normal" scan delusion
In an era of high-tech diagnostics, clinicians are often conditioned to wait for CT or MRI confirmation before initiating treatment. For gas embolisms, this instinct can be fatal. Radiographic imaging should never be used to exclude a diagnosis of AGE.
The source evidence is clear: brain imaging is frequently normal, even when severe neurological abnormalities are present. Waiting for a scan can dangerously delay the only definitive treatment: hyperbaric oxygen (HBO2) therapy. However, there is one critical caveat - while brain scans are often useless for diagnosis, a chest radiograph or ultrasound is a vital "pre-chamber" check. This is necessary to exclude a pneumothorax, which could expand into a life-threatening tension pneumothorax during the decompression phase of hyperbaric treatment.
The primary reason to perform a brain scan is not to find bubbles, but to rule out other conditions. As the clinical guidelines state:
"The only rational reason to perform diagnostic imaging is to exclude other pathology that might have similar manifestations as AGE but require different management (e.g., intracranial haemorrhage)."
3. The household hazard: hydrogen peroxide
One of the most impactful causes of gas embolism has no connection to diving or surgical suites; it involves the ingestion of hydrogen peroxide. Once swallowed, the chemical is absorbed into the portal circulation, where it interacts with the enzyme catalase in erythrocytes (red blood cells) to release massive volumes of gaseous oxygen directly into the bloodstream.
This mechanism carries unique risks. While diving-related AGE presents in seconds, peroxide-induced embolisms can have a significantly delayed onset, with symptoms appearing anywhere from 24 to 72 hours after ingestion. Furthermore, this "slow-burn" emergency is often accompanied by visceral complications; the source notes that 27 of 49 patients with portal venous gas from peroxide ingestion also experienced significant gastrointestinal (GI) bleeding.
4. Why "head-down" is no longer the standard
For decades, the Trendelenburg (head-down) position was the standard first-aid protocol, based on the theory that buoyancy would prevent bubbles from floating into the brain. Current medical evidence has officially overturned this practice. Research demonstrates that buoyancy has a negligible effect on the distribution of intravascular air. Moreover, the head-down position is now known to worsen cerebral oedema (brain swelling).
The current evidence-based standard is the supine position (lying flat). For unconscious patients, the lateral decubitus (recovery) position is used to protect the airway. Critically, clinicians must be wary of "postural change" during transport. The source warns that re-embolisation can occur when a patient is moved from a supine to an upright position, as previously sequestered bubbles in "anatomic traps" like the pulmonary veins may be released back into the circulation.
5. The "time machine" effect of hyperbaric hyperoxia
While early intervention is the gold standard, HBO2 therapy offers a remarkable "time machine" effect, remaining effective 24 hours or more after the initial event. This is because the mechanical reduction of bubble volume is only part of the therapeutic equation.
The real "magic" lies in the pharmacological effects of hyperbaric hyperoxia. Intravascular bubbles do more than just block flow; they damage the vessel lining by stripping the endothelium from the underlying basement membrane and triggering TRPV ion channels, which leads to calcium entry and cell death. HBO2 works by inhibiting leukocyte (white blood cell) adhesion to this damaged endothelium, effectively halting the secondary inflammatory cascade and restoring blood flow.
The resilience of the human brain under these conditions is extraordinary, provided clinical suspicion remains high. Consider the case of a 51-year-old diver:
"[The patient] lost consciousness within minutes of a 30-metre dive... remained deeply comatose for six days, intubated and with cardiovascular instability before HBO2 could be administered. One year after treatment he was leading a functional life."
Conclusion: clinical suspicion over technology
The management of gas embolisms has evolved from a simple mechanical focus on "shrinking bubbles" to a sophisticated understanding of complex inflammatory management. We now know that the danger can be shallow, the brain scans can be misleading, and the treatment window is wider than once believed.
In our current medical landscape, the most powerful tool for survival is not the scanner, but the doctor's intuition. By prioritising immediate, evidence-based action over technological confirmation, we honour the incredible resilience of the human brain and the life-saving necessity of rapid clinical suspicion.
This feature article is general educational information and does not replace advice from your own doctor or emergency services. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.