Hyperbaric Oxygen Therapy for Crush Injury
After a severe crush injury, swelling can starve the tissue of oxygen. Given early and alongside surgery, hyperbaric oxygen helps support injured-but-salvageable tissue in crush injury, compartment syndrome and other acute traumatic ischaemias.
What this means for you
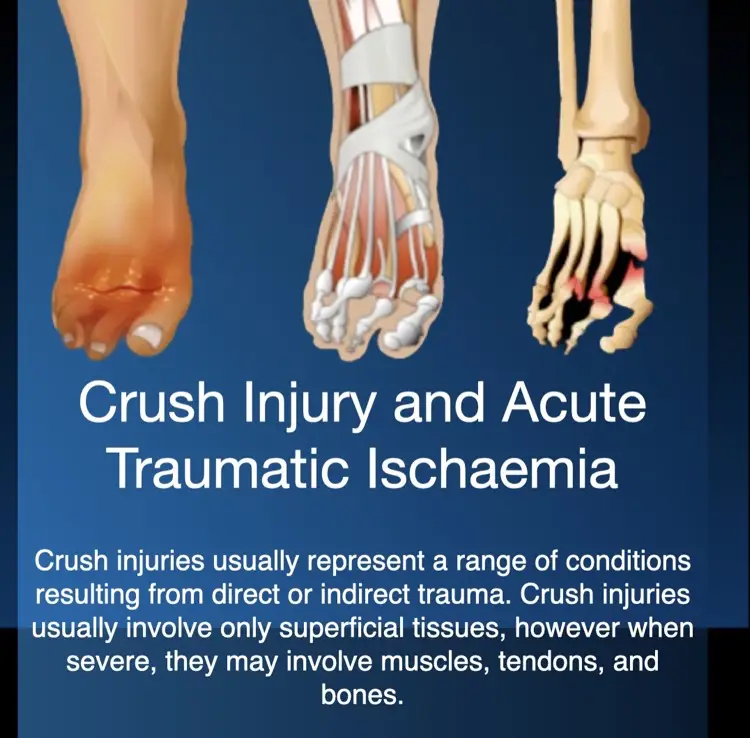
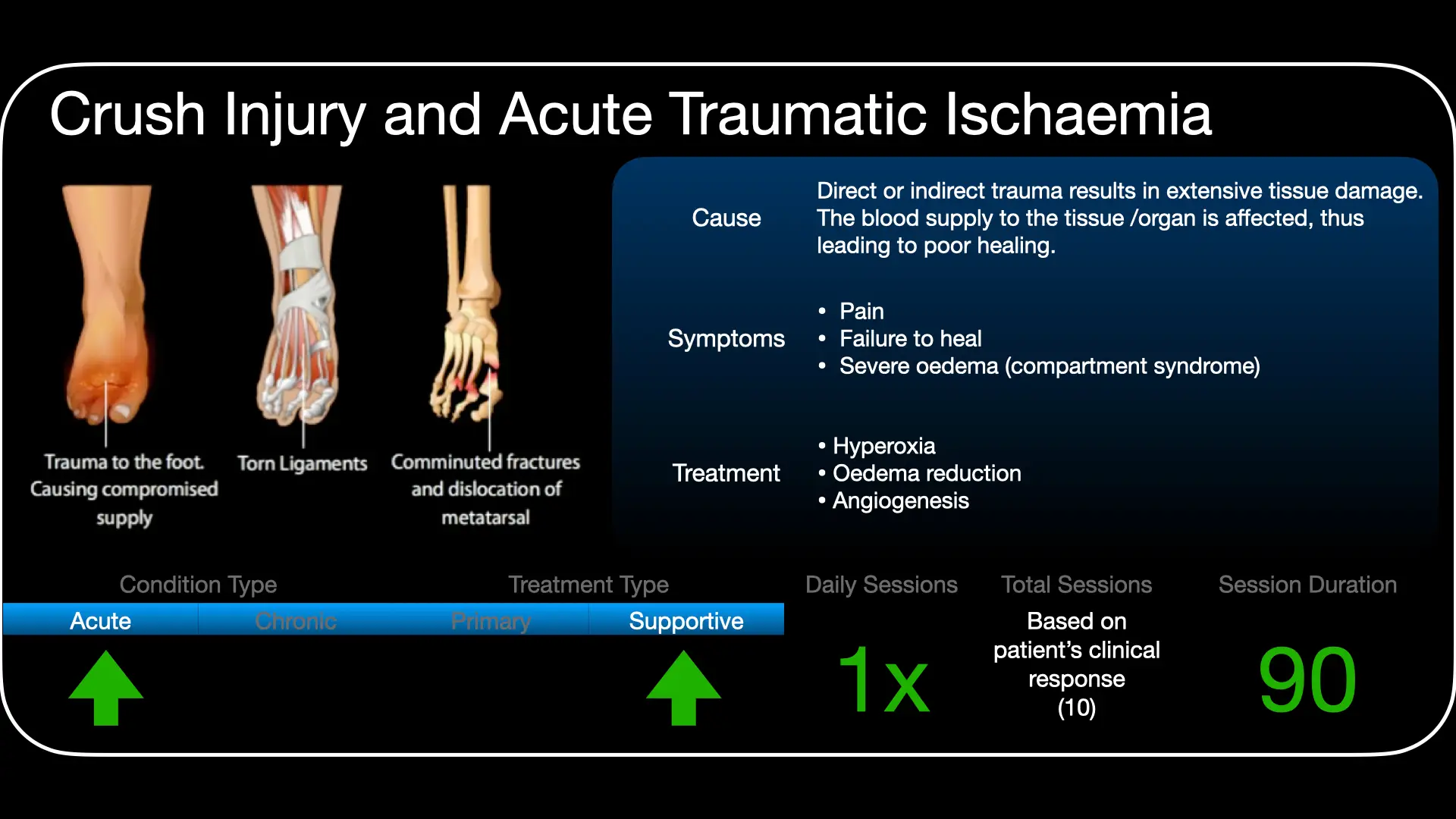
What is a crush injury?
A crush injury happens when part of the body is squeezed or crushed with great force - for example in a road or industrial accident. Besides broken bones and torn tissue, the injured area swells. Because muscle sits in tight compartments, that swelling can squeeze shut the small blood vessels and cut off the oxygen supply - a problem called compartment syndrome, and part of a group of conditions called acute traumatic ischaemias.
Why does the oxygen supply matter?
Around the obviously damaged tissue there is often a border of tissue that is injured but still alive. If it does not get enough oxygen quickly, it can be lost - leading to wound problems, repeat operations, and in severe cases the risk to the limb. The aim is to protect that borderline tissue.
How can hyperbaric oxygen help?
Used early and together with surgery, hyperbaric oxygen raises the oxygen reaching the injured area and helps reduce swelling. In the chamber you breathe pure oxygen under pressure, which dissolves extra oxygen into the blood so it can reach tissue with a squeezed blood supply. This can support the borderline tissue and may lower the risk of wound complications and further surgery.
What to expect
When used for a crush injury, hyperbaric oxygen is started early and given as repeated sessions over the first days, coordinated around your operations and other treatment. Whether it is suitable depends on the type and severity of the injury and your overall condition.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Breathing Under Pressure (English)
Breathing Under Pressure (English) Die Bose Kringloop (Afrikaans)
Die Bose Kringloop (Afrikaans) For Patients: Acute Traumatic Ischaemias (UHMS 06)
For Patients: Acute Traumatic Ischaemias (UHMS 06)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Crush injury, compartment syndrome and other acute traumatic ischaemias are a recognised indication for adjunctive hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO is a time-sensitive adjunct to definitive orthopaedic and vascular management - fracture stabilisation, fasciotomy and revascularisation as indicated.
Rationale
Severe traumatic ischaemia combines mechanical tissue disruption with progressive oedema, raised compartment pressures, microvascular compromise and ischaemia-reperfusion injury. As with the burn, there is a zone of marginally perfused but viable tissue whose survival depends on restoring oxygen delivery before irreversible loss occurs.
Mechanisms
HBO sharply raises plasma-dissolved oxygen, oxygenating tissue whose capillary supply is compromised by oedema. Hyperoxic vasoconstriction reduces oedema (and compartment pressures) without lowering oxygen delivery, it attenuates ischaemia-reperfusion injury by reducing neutrophil adhesion and the no-reflow phenomenon, and it supports cellular energetics and the microcirculation - collectively limiting secondary tissue loss and supporting wound healing.
Role in management
- Adjunct only, and early: benefit is greatest when started within hours; it does not replace fasciotomy, fixation or revascularisation.
- Greatest value in severe injuries (e.g. Gustilo grade III open fractures) and threatened marginal tissue.
- Coordinate with orthopaedics/vascular surgery and intensive care; manage rhabdomyolysis and renal protection in crush syndrome separately.
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.5 ATA, given more frequently in the first 24-48 hours and then reducing, over a short early course guided by clinical response. Exact pressures, durations and frequency are individualised and set case by case at the unit.
Evidence base
The randomised evidence is modest but consistent in direction, and we present it honestly. The double-blind Bouachour trial (1996) in severe limb crush injury found better wound healing and fewer repeat operations with early adjunctive HBO, with the benefit concentrated in patients over 40 and in the most severe (Gustilo III) injuries. The larger, more recent HOLLT trial (Millar 2022, 120 open tibial fractures) missed its primary composite endpoint (necrosis/infection at 14 days, p=0.12) but showed significantly less tissue necrosis (29% vs 53%), fewer late complications, and better 1–2 year function. Time to first treatment is the key modifiable factor - benefit is greatest when HBO starts within about 4–6 hours of injury.
The mechanism is well characterised in animal and laboratory work (Strauss; Oyaizu): HBO reduces tissue oedema through hyperoxic vasoconstriction while keeping the marginally perfused "zone of stasis" oxygenated, limits reperfusion injury, and accelerates muscle regeneration. A recent 145-patient earthquake cohort (Kılınç 2025) found early fasciotomy essential and HBO independently associated with better functional recovery, though this is observational. HBO is a recognised UHMS indication used as a time-critical adjunct to surgery.
Bottom line
HBO never replaces or delays surgery - fasciotomy for compartment syndrome, and vascular repair, come first. Added early (ideally within 4–6 hours) as an adjunct, it can reduce oedema, limit tissue loss in the zone of stasis, and support limb salvage in severe crush injury. The evidence is limited but consistent; the benefit is greatest in the most severe injuries and when treatment starts promptly.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 06 — Acute Traumatic Ischaemias
UHMS Indications, Ch. 06 — Acute Traumatic Ischaemias HMP, Ch. 26 — HBO in Crush Injury & Acute Traumatic Ischaemias
HMP, Ch. 26 — HBO in Crush Injury & Acute Traumatic Ischaemias HBOT for Crush Injuries (overview)
HBOT for Crush Injuries (overview) Crush Syndrome (talk)
Crush Syndrome (talk)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Crush Injury, Compartment Syndrome and Other Acute Traumatic Ischaemias.
- Bouachour G, Cronier P, Gouello JP, et al. Hyperbaric oxygen therapy in the management of crush injuries: a randomized double-blind placebo-controlled clinical trial. J Trauma. 1996;41(2):333-9.
- Millar IL, et al. Hyperbaric Oxygen for Lower Limb Trauma (HOLLT): an international multi-centre randomised clinical trial. Diving Hyperb Med. 2022;52(3):164-74.
- Strauss MB, Hargens AR, Gershuni DH, et al. Reduction of skeletal muscle necrosis using intermittent hyperbaric oxygen in a model compartment syndrome. J Bone Joint Surg Am. 1983;65(5):656-62. doi:10.2106/00004623-198365050-00011
- Oyaizu T, Enomoto M, Yamamoto N, et al. Hyperbaric oxygen reduces inflammation, oxygenates injured muscle, and regenerates skeletal muscle via macrophage and satellite cell activation. Sci Rep. 2018;8(1):1288. doi:10.1038/s41598-018-19670-x
- St. Pierre Schneider B, Zhang L, Dombrowsky T, Wilson JR. A scoping review and evaluation of hyperbaric oxygen therapy for skeletal muscle injury in preclinical models. Med Gas Res. 2026;16(2):125-32. doi:10.4103/mgr.MEDGASRES-D-24-00163
- Kılınç O, Günaydın F, Sakarya B, et al. The effect of fasciotomy timing on limb vitality and functionality in Kahramanmaraş/Turkey earthquake. Acta Orthop Belg. 2025;91(4):495-502. doi:10.52628/91.4.14579
The Invisible Scalpel: How Hyperbaric Oxygen is Quietly Revolutionising Trauma Recovery
The high stakes of acute trauma
Traumatic injuries are not merely personal tragedies; they are a staggering systemic crisis. In 2016 alone, the National Trauma Organization reported a gargantuan $672 billion spent on trauma care - a figure that ignores the unquantifiable costs of lost income and lifelong psychological scars. Yet, despite this half-trillion-dollar investment, complication rates for the most severe orthopaedic injuries, such as Gustilo Grade III B and C open fractures, remain stubbornly fixed at 50%.
At the centre of this failure is "acute traumatic ischaemia." This is not a static injury but a dynamic crisis of oxygen delivery. In the wake of trauma, the body's sophisticated transport systems break down, leading to a desperate state where cells suffocate in silence. It raises a provocative question for modern medicine: how can a simple element - oxygen - when pressurised in a hyperbaric chamber, salvage results where state-of-the-art surgery alone fails?
Oxygen that bypasses the red blood cell
The primary "magic trick" of hyperbaric oxygen (HBO2) therapy is a pivot from biology to physics. Under normal atmospheric conditions, oxygen is the passenger of the red blood cell (erythrocyte). In acute trauma, however, the microcirculation often collapses or "sludges", creating a cellular traffic jam that prevents these red blood cells from reaching the wounded tissue.
HBO2 bypasses this bottleneck by significantly increasing the amount of physically dissolved oxygen directly in the plasma. This turns the plasma itself into a high-octane delivery vehicle that can reach tissues even when the flow of red blood cells is completely blocked.
"With HBO2, oxygen becomes no more flow dependent than the other dissolved substances in the plasma."
By making oxygen delivery independent of erythrocyte flow, HBO2 ensures that survival-critical "payloads" reach tissues where the traditional biological transport system has effectively ceased to function.
The paradox of the inflammatory stage
The biological narrative of trauma contains a cruel irony during the "inflammatory stage." This phase begins the moment of impact and represents the exact window when the body's oxygen requirements are at their absolute peak. Oxygen is the fuel required to mobilise growth factors and leukocytes to combat infection and initiate repair.
Paradoxically, this is the exact moment when the tissue has the least oxygen available. The energy exchange from the trauma causes immediate oedema, vascular damage, and vasospasms. The wound is essentially suffocating at the very second it needs to breathe most. By initiating HBO2 early in this stage, clinicians can mitigate these hypoxia-associated effects before the cellular damage becomes irreversible.
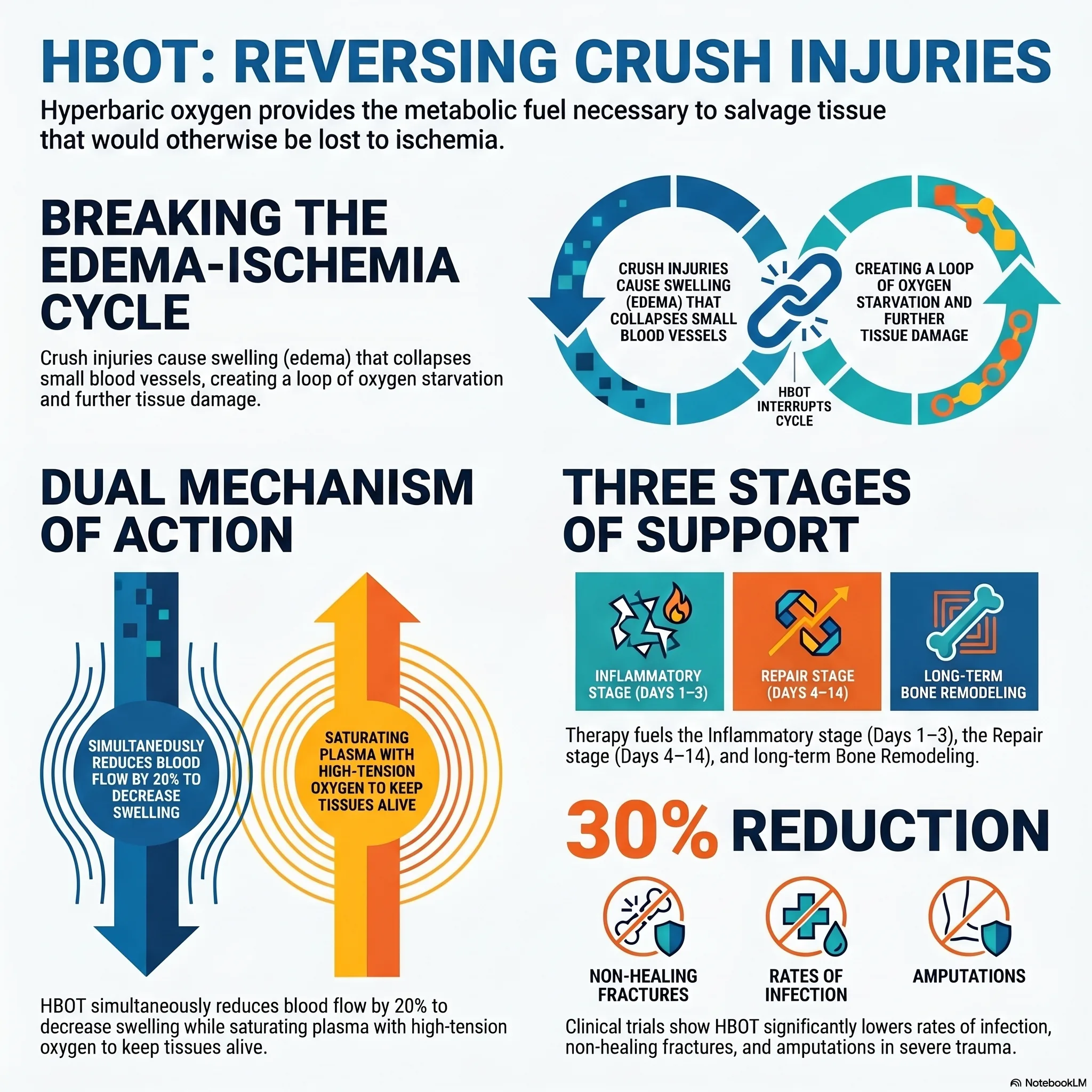
Drying the wound: breaking the "death spiral"
When tissue is injured, it enters a self-perpetuating "death spiral" known as the oedema, ischaemia-hypoxia cycle. The initial injury causes swelling (oedema), which increases the distance oxygen must travel from capillaries to cells. This pressure can collapse the microcirculation entirely, further starving the cells. Starved cells then lose the ability to maintain their intracellular water balance, causing even more swelling.
HBO2 is the only intervention that interrupts this cycle while simultaneously optimising oxygen availability through a dual mechanism:
- 20% vasoconstriction: it triggers pre-injury arteries and arterioles to constrict, reducing the inflow of fluid and "drying out" the oedema.
- Hyper-oxygenation: despite the reduced blood flow, the oxygen tension in the plasma is so high that the tissue receives a massive surplus of oxygen compared to normal conditions.
By reducing the pressure of the swelling while maximising the oxygen payload, HBO2 effectively stabilises the tissue's environment, allowing the repair stage - driven by fibroblasts and macrophages - to begin on a solid foundation.
The "lag phase" and the golden window
In skeletal muscle-compartment syndrome (SMCS), the stakes are defined by the "lag phase." This is the window between the initial blunt trauma and the moment intracompartmental pressure exceeds capillary perfusion pressure, leading to total motor loss and severe pain.
During this phase, the diagnosis is often elusive. However, data suggests that early intervention during this window is revolutionary. In a retrospective finding (Strauss, 1981), the frequency of early HBO2 was the single greatest predictor of success. While three treatments yielded 80% positive outcomes, six treatments in the first 24 hours generated 100% positive outcomes. In cases of SMCS specifically, no patient in the "lag phase" progressed to a fasciotomy when HBO2 was started early.
The 30% efficiency gain: burns and grafts
The transformative power of HBO2 is perhaps most visible in the treatment of thermal burns and threatened flaps. By utilising the American Burn Association's classification system, researchers have identified that for deep partial-thickness and full-thickness burns, HBO2 acts as a powerful stabilising force.
The data reveals a consistent "30% efficiency gain": a 30% reduction in fluid loss and a 30% decrease in the need for skin grafts. For the patient and the hospital, this translates to a one-third reduction in the length of stay. In cases of compromised re-implantations where venous congestion threatens the limb, HBO2 even works in tandem with ancient-yet-effective tools like leeches - using vasoconstriction to reduce congestion while the leeches manage the outflow.
The "Wellness Score" vs. "que sera sera"
In the high-pressure environment of trauma surgery, decisions are often subjective. Some surgeons adopt a "que sera sera" (whatever will be, will be) attitude, viewing complications as an unavoidable part of the process. To combat this, innovative clinicians are moving toward rationale-based indications (RBI) and objective scoring tools like the "Wellness Score."
Because only 20% of clinical decisions in medicine are backed by randomised controlled trials, the Wellness Score provides a pragmatic framework for deciding between limb salvage and primary amputation.
| Assessment | 2 points | 1 point | 0 points |
|---|---|---|---|
| Activities of daily living | Full | Some | None |
| Ambulation | Community | Household (subtract ½ if aids used) | None |
| Comorbidities | None significant | Impaired | Decompensated |
| Inhibitors | None | Past (smoking / immunosuppressors) | Current |
| Neurological deficits | None | Some / minor (sensation / balance) | Major (paralysis / cognitive) |
Note on scoring: total scores of 7.5-10 indicate a "healthy" host; 3.5-7 indicate "impaired"; 0-3 indicate "decompensated."
Conclusion: the 5% dilemma
The evidence is categorical: hyperbaric oxygen is not a mere "adjunct" but a specific intercessor for the pathophysiology of trauma. It is a biological bridge that carries tissue through the most dangerous stages of healing.
However, a massive dilemma remains. Of the approximately 1,500 hyperbaric facilities in the United States, only an estimated 70 (about 5%) are equipped or willing to handle these acute emergencies. The vast majority are restricted to stable, outpatient wound care. This gap is driven by a lack of "cutouts" in reimbursement - Medicare and private insurers rarely cover HBO2 for acute trauma admissions, discouraging hospitals from maintaining 24/7 emergency hyperbaric capabilities.
We are left with a haunting reality: we have a tool that can reduce complications by 30% and save thousands of limbs every year, yet it remains locked behind administrative and reimbursement hurdles. As we continue to spend $672 billion annually on trauma, we must ask ourselves why we accept a 50% complication rate as the status quo when the "invisible scalpel" is waiting just out of reach.
This feature article is general educational information and does not replace advice from your own doctor or emergency services. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.