Hyperbaric Oxygen Therapy for Complex Wounds
Some wounds - such as certain diabetic foot ulcers - struggle to heal because the tissue lacks oxygen. For selected wounds, hyperbaric oxygen is used alongside good wound care to support healing.
What this means for you
What is a complex or non-healing wound?
Most wounds heal on their own within a few weeks. Some do not - they get stuck and stay open for months. This often happens when the blood and oxygen supply to the area is poor, when diabetes affects healing, or when infection or past radiation is involved. Diabetic foot ulcers are one of the commonest examples. These "problem wounds" need extra help.
How can hyperbaric oxygen help?
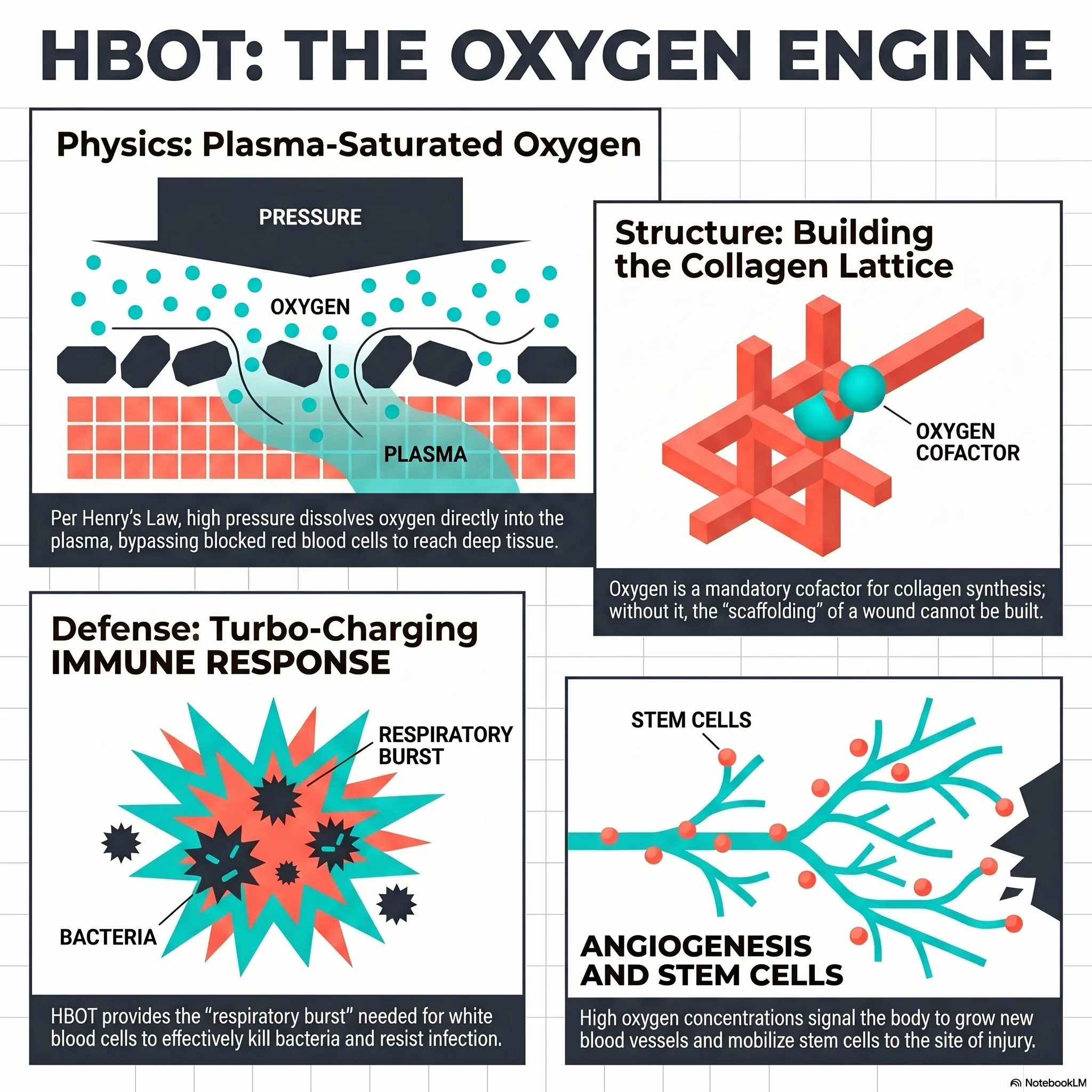
Healing tissue is hungry for oxygen - it needs oxygen to fight infection, to build new tissue, and to grow new blood vessels. In the hyperbaric chamber you breathe pure oxygen under pressure, which greatly increases the oxygen delivered to the wound. In selected wounds, this can help re-start healing that has stalled.
What to expect
If hyperbaric oxygen is suitable for your wound, it is given as a course of regular sessions over several weeks, alongside the rest of your wound care. Your wound and circulation are assessed first to decide whether it is likely to help. We also use a test called transcutaneous oximetry (TcPO₂) to measure the oxygen around a wound.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Healing Under Pressure (English)
Healing Under Pressure (English) Druk-genesing: Probleemwonde (Afrikaans)
Druk-genesing: Probleemwonde (Afrikaans) For Patients: Selected Problem Wounds (UHMS 02b)
For Patients: Selected Problem Wounds (UHMS 02b)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Selected problem wounds - most notably diabetic foot ulcers (Wagner grade 3 or higher) that have failed to respond to a period of optimal standard care - are a recognised indication for adjunctive hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO supplements, and never replaces, comprehensive wound management.
Rationale
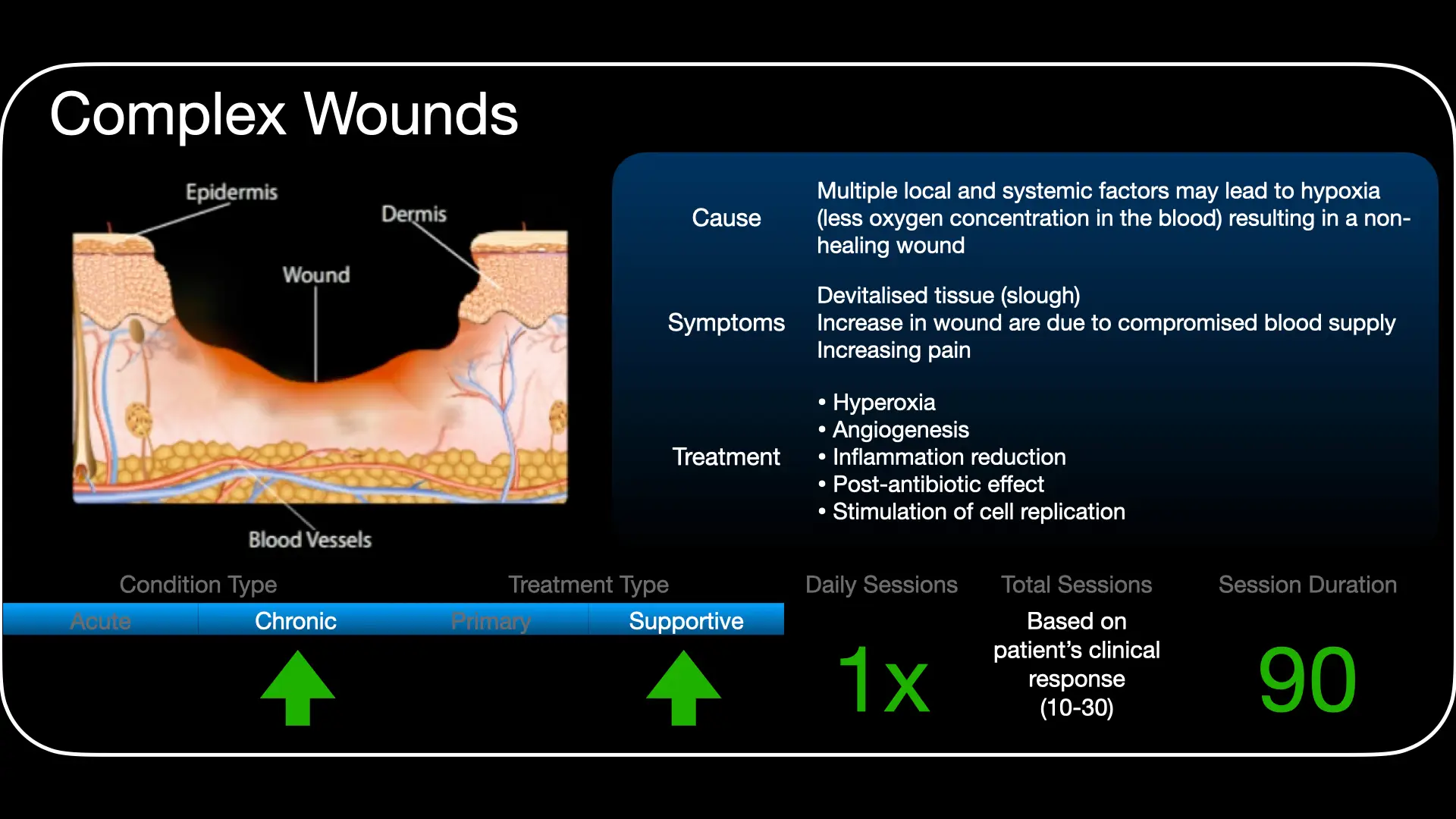
Chronic wounds are characterised by persistent tissue hypoxia, impaired neutrophil oxidative killing, deficient angiogenesis and stalled fibroplasia. Wound healing is oxygen-dependent at almost every step. Intermittent hyperoxia aims to correct the hypoxic bottleneck and restore the cellular processes of repair in tissue that has adequate, or restorable, macrovascular inflow.
Mechanisms & selection
HBO raises wound-tissue oxygen tensions far above baseline, restoring oxygen-dependent leukocyte bactericidal activity, fibroblast proliferation and collagen synthesis, and growth-factor-driven angiogenesis. Crucially, large-vessel perfusion must be adequate or revascularised first - HBO cannot compensate for uncorrected macrovascular disease. Transcutaneous oximetry (TcPO₂), including in-chamber response, helps select likely responders.
Role in management
- Adjunct only: debridement, offloading, moisture balance, infection control, glycaemic optimisation and vascular assessment/revascularisation come first.
- Assess perfusion (ABI/toe pressures, TcPO₂); correct ischaemia before or alongside HBO.
- Reassess response objectively; discontinue if the wound is not progressing.
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.5 ATA, once daily, over a course typically in the order of 20-40 sessions, with the wound reviewed for objective progress. Exact protocol is individualised and set case by case at the unit.
Evidence base
Diabetic foot ulcers (DFU) are the best-studied wound indication. The double-blind HODFU trial (Löndahl 2010) reported complete healing at one year in 52% with HBO versus 29% with sham (number-needed-to-treat about 4), and an ischaemic-DFU trial (Faglia 1996) reduced major amputation from 33% to 9% (relative risk 0.26). Meta-analyses (Cochrane; Kranke 2015) pool lower major-amputation odds and improved short-term healing, and an independent GRADE review (Goldman 2009) graded the amputation evidence in infected DFU as high. A Canadian cost-effectiveness model (Chuck 2008) found adjunctive HBO cost-saving and more effective over 12 years, driven by avoided amputations.
The evidence is genuinely mixed, and we present it that way. Two later double-blind RCTs were negative - Fedorko 2016 (no reduction in amputation) and the DAMOCLES trial (Santema 2018) in ischaemic ulcers - and the largest observational study (Margolis 2013, 6,259 patients) found no benefit once patient selection was accounted for. The consistent signal across positive and negative studies is that response depends on selection: transcutaneous oximetry (TcPO₂) identifies the hypoxic, hyperoxia-responsive wounds that benefit. HBO is therefore a selective adjunct within a structured wound-care pathway - never a substitute for offloading, debridement, infection control, glycaemic control or revascularisation.
Bottom line
In well-selected patients - chronic, hypoxic, TcPO₂-responsive wounds that have failed standard care - adjunctive HBO improves healing and reduces major amputation. In unselected use the benefit disappears. It complements, and never replaces, wound care, offloading, infection control and revascularisation.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 02b — Selected Problem Wounds
UHMS Indications, Ch. 02b — Selected Problem Wounds HMP, Ch. 23 — Adjunctive HBOT for Diabetic Foot Ulcers
HMP, Ch. 23 — Adjunctive HBOT for Diabetic Foot Ulcers HBOT for Selected Problem Wounds (overview)
HBOT for Selected Problem Wounds (overview)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Enhancement of Healing in Selected Problem Wounds.
- Löndahl M, Katzman P, Nilsson A, Hammarlund C. Hyperbaric oxygen therapy facilitates healing of chronic foot ulcers in patients with diabetes. Diabetes Care. 2010;33(5):998-1003.
- Faglia E, Favales F, Aldeghi A, et al. Adjunctive systemic hyperbaric oxygen therapy in treatment of severe prevalently ischemic diabetic foot ulcer. Diabetes Care. 1996;19(12):1338-43.
- Kranke P, Bennett MH, Martyn-St James M, et al. Hyperbaric oxygen therapy for chronic wounds. Cochrane Database Syst Rev. 2015;(6):CD004123.
- Goldman RJ. Hyperbaric oxygen therapy for wound healing and limb salvage: a systematic review. PM&R. 2009;1(5):471-89.
- Fedorko L, Bowen JM, Jones W, et al. Hyperbaric oxygen therapy does not reduce indications for amputation in patients with diabetes with nonhealing ulcers of the lower limb: a randomized controlled clinical trial. Diabetes Care. 2016;39(3):392-9.
- Santema KTB, Stoekenbroek RM, Koelemay MJW, et al. Hyperbaric oxygen therapy in the treatment of ischemic lower-extremity ulcers in patients with diabetes (DAMOCLES). Diabetes Care. 2018;41(1):112-9.
- Margolis DJ, Gupta J, Hoffstad O, et al. Lack of effectiveness of hyperbaric oxygen therapy for the treatment of diabetic foot ulcer and the prevention of amputation: a cohort study. Diabetes Care. 2013;36(7):1961-6.
- Chuck AW, Hailey D, Jacobs P, Perry DC. Cost-effectiveness and budget impact of adjunctive hyperbaric oxygen therapy for diabetic foot ulcers. Int J Technol Assess Health Care. 2008;24(2):178-83.
The Underwater Origin and Turbocharged Future of Wound Healing: 6 Insights from Hyperbaric Medicine
In an era of CRISPR and robotic surgery, the "problem wound" remains a humbling adversary - a biological stalemate where the body simply forgets how to repair itself. When standard care reaches a plateau of metabolic surrender, the stalled healing process is often more than a clinical failure; it is a sign that the cellular machinery has run out of its most fundamental fuel.
Hyperbaric oxygen therapy (HBO2) is frequently dismissed as the simple act of "breathing more air." In reality, it is a sophisticated biological intervention that leverages environmental pressure to "re-prime" the body's internal engine. By exploring the frontiers of undersea and hyperbaric medicine, we find that the future of regenerative care is being written by the laws of gas and physiology.
1. Healing lessons from Jacques Cousteau's divers
Modern wound care owes an ironic debt to the high-pressure maritime environments of the mid-20th century. While living 35 feet beneath the surface of the Red Sea, Jacques Cousteau's divers reported a strange phenomenon: their minor cuts and abrasions healed with startling speed while they inhabited their underwater habitat.
This maritime anecdote was eventually validated in 1964, when the National Science Foundation commissioned Dr T K Hunt to investigate the divers' claims. His subsequent research provided the scientific bedrock for the field, proving that wound healing is strictly oxygen-dependent. There is a profound irony in our high-tech hyperbaric suites; we are essentially building land-locked machines to replicate the "high-pressure soup" of the Red Sea that Cousteau's pioneers first discovered.
2. Oxygen functions as a high-tech antibiotic
We traditionally view antibiotics as chemical agents - pills or intravenous fluids. However, in the context of hyperbaric medicine, oxygen serves as a critical co-factor in the body's innate antimicrobial defence system. Immune cells known as neutrophils require oxygen to produce reactive oxygen species (ROS), such as hydrogen peroxide, to neutralise bacteria - a process known as "oxidative killing."
In a hypoxic wound, the immune system's ammunition literally runs out. While "non-oxidative" pathways can manage less virulent bacteria, they are no match for the aggressive species that thrive in the stagnant environments of chronic ulcers. As the clinical evidence makes clear:
"Oxygen metabolism is a critical co-factor in many cellular processes from collagen deposition to antimicrobial activity... intracellular leukocyte bacterial killing [is an] oxygen-sensitive process that is essential to wound healing."
3. The "NOS" effect - turbocharging the healing engine
In high-performance racing, a nitrous oxide system (NOS) provides a temporary, massive boost to an engine's power. HBO2 performs a nearly identical function for the cellular machinery, but the connection is more than just metaphorical. HBO2 activates the enzyme nitric oxide synthase (NOS), providing the biological "turbo-boost" necessary to mobilise stem cells and move them to the site of injury.
While normobaric oxygen (100% O2 at sea level) has minimal effect on gene expression, hyperbaric pressure has been shown to upregulate over 8,000 genes. This includes the massive synthesis of critical growth factors and receptors that are essential for building new tissue:
- VEGF (vascular endothelial growth factor)
- bFGF (basic fibroblast growth factor)
- TGF-β1 (transforming growth factor beta-1)
4. The TcPO2 "crystal ball"
Bio-innovation is only as good as its predictive accuracy. Transcutaneous oxygen measurement (TcPO2) acts as a physiological crystal ball, allowing clinicians to determine which wounds are likely to respond before committing to weeks of therapy. However, the true predictive power lies not in room-air measurements, but in "in-chamber" data.
This is a tunable process. If a patient does not reach the therapeutic "Rule of 200" (an in-chamber TcPO2 of >200 mmHg) at 2.0 ATA, the clinician can "crank up" the pressure to 2.4 ATA. The difference is stark: patients who hit that 200 mmHg mark have an 84% likelihood of benefit, while those who remain below 100 mmHg have only a 14% chance of success. This allows the hyperbaric chamber to function as a tunable diagnostic tool rather than a static box.
5. Why "VOIDS" is more important than the chamber
Despite the high-tech nature of the chamber, HBO2 is never a monotherapy; it is a "team sport." The technology is only as effective as the multidisciplinary "foot team" supporting it. The secret sauce of the landmark Italian studies led by pioneers like Faglia and Baroni was not just the pressure, but the integration of HBO2 with aggressive revascularisation and the "VOIDS" protocol:
- Vascular optimisation
- Off-loading
- Infection control
- Diabetes control
- Surgical debridement
The Italian researchers proved that HBO2 combined with aggressive surgical and metabolic management is what drives superior outcomes. The chamber provides the substrate, but the team ensures the substrate is not wasted.
6. The economic argument for "expensive" air
At roughly $50,000 for a full course, HBO2 is often criticised as an expensive luxury. However, it is "economically dominant" - meaning it costs less and provides better outcomes than the alternative. Contrast the $50,000 investment against the $66,000 to $73,000 cost of a major amputation (below-knee or above-knee).
The argument isn't just about the balance sheet; it's about survival. Historical data reveals a harrowing 47.2% mortality rate for amputation controls, compared to 35.4% for those on limb-salvage protocols. By investing in hyperbaric treatment, healthcare systems aren't just saving money - they are literally buying time and quality-adjusted life-years (QALYs) for their patients. In the long run, "expensive air" is the only thing we can't afford to ignore.
Conclusion: the fluctuation of life
The true power of hyperbaric medicine lies in the "pumping action" of intermittent hyperoxia. By swinging the body between high and low oxygen states, HBO2 mimics the momentum of a child on a swing, providing the biological "push" needed to restart a stalled engine.
As we look toward the future of regenerative medicine, we must ask: if we can "re-prime" the body's healing engine through the precise application of pressure and gas, what other "incurable" conditions might eventually yield to the laws of physiology?
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.