Hyperbaric Oxygen Therapy for Central Retinal Artery Occlusion
Central retinal artery occlusion (CRAO) is a "stroke of the eye" - a sudden, painless loss of vision and a time-critical emergency. Hyperbaric oxygen can keep the retina alive while the blockage is treated.
What this means for you
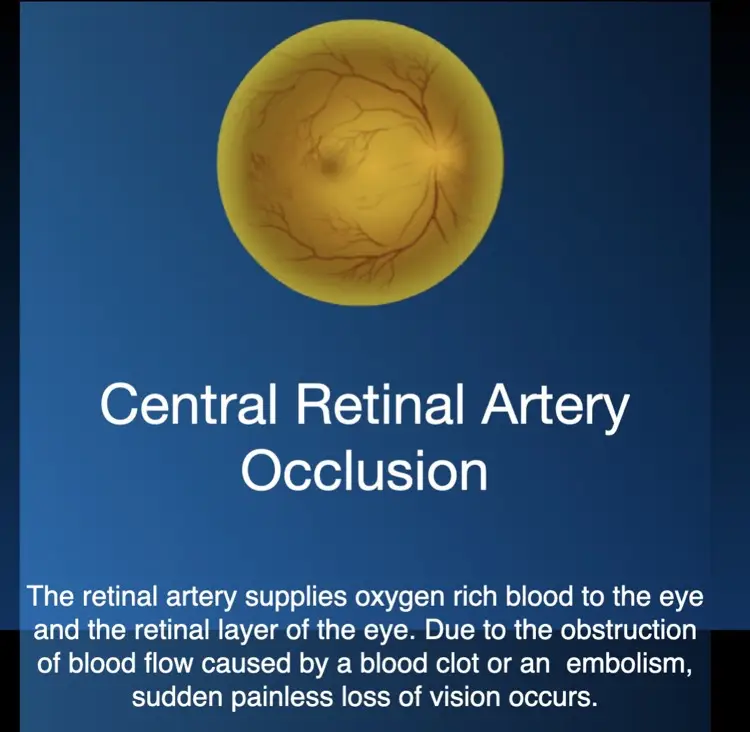
What is central retinal artery occlusion?
The retina is the light-sensitive layer at the back of the eye, and it is fed by a single main artery. If that artery suddenly becomes blocked - usually by a clot or debris - the retina is starved of oxygen and vision in that eye is lost, almost always without pain. Because it is the eye's equivalent of a stroke, it is often called a "stroke of the eye".
How can hyperbaric oxygen help?
Even when the main artery is blocked, the retina can still absorb oxygen from a second layer of blood vessels just behind it - but only if the oxygen level in the blood is raised very high. In the hyperbaric chamber you breathe pure oxygen under pressure, which floods the blood with oxygen and can keep the retina alive while the blockage is treated, giving your vision the best possible chance to recover. The earlier it is started, the better.
Why you also need a stroke check-up
Because CRAO usually has the same causes as a brain stroke, it is an important warning sign. Alongside treating your eye, you will need an urgent check of your heart and the blood vessels to your brain, to lower the risk of a stroke or heart attack in the days that follow.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 A Stroke of the Eye (English)
A Stroke of the Eye (English) 'n Beroerte van die Oog (Afrikaans)
'n Beroerte van die Oog (Afrikaans) For Patients: CRAO (UHMS 2a)
For Patients: CRAO (UHMS 2a) For Patients: CRAO Protocol 2025
For Patients: CRAO Protocol 2025This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
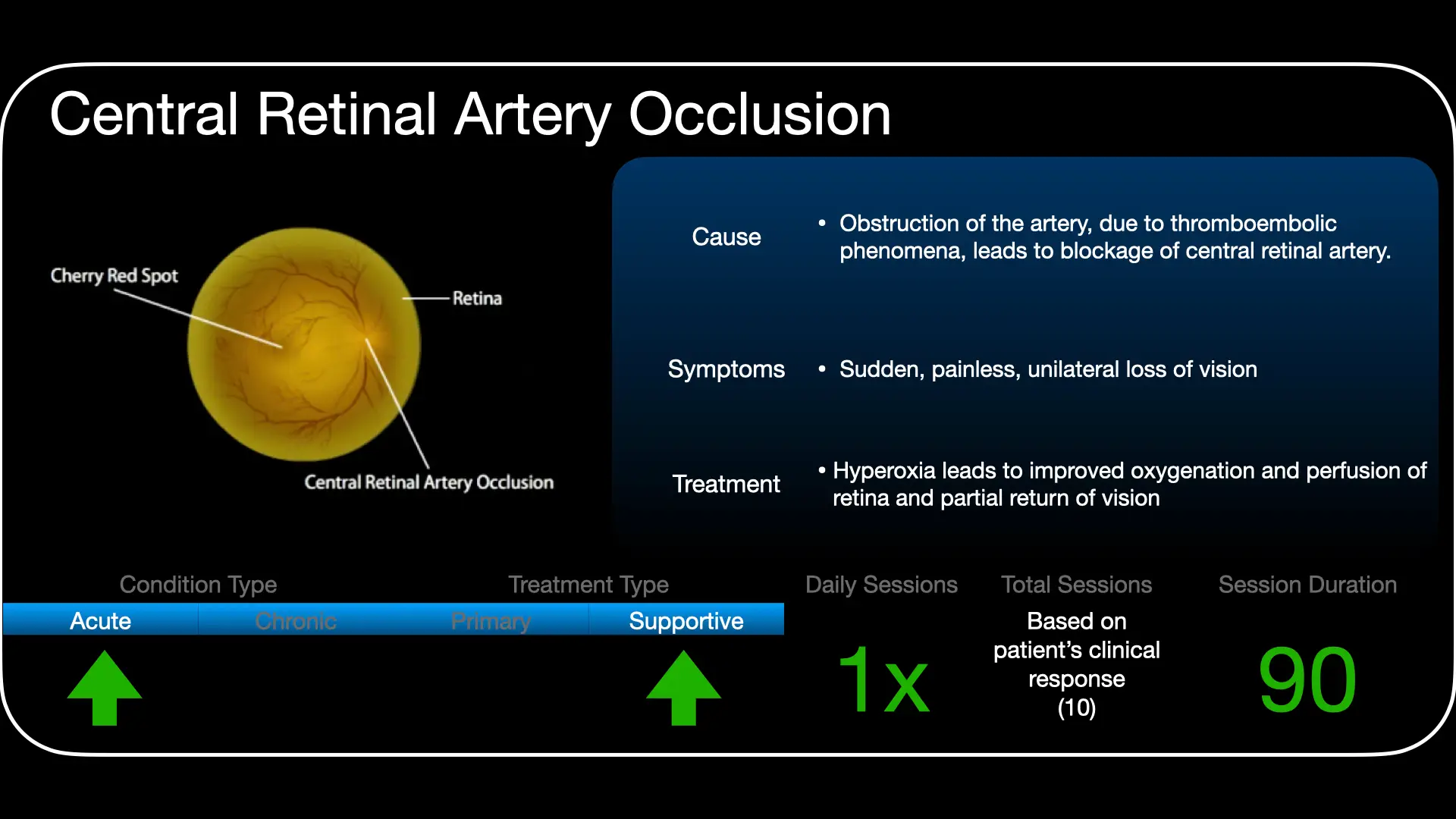
Acute, non-arteritic central retinal artery occlusion (CRAO) is a recognised indication for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). It is a true ocular emergency and a central-nervous-system ischaemic event - a stroke equivalent - so treatment is time-critical and must be paired with urgent stroke evaluation.
Rationale
The inner retina is supplied by the central retinal artery, but the outer retina is supplied by the choroid (posterior ciliary circulation). At normal arterial oxygen tensions the choroid cannot oxygenate the inner retina across the occlusion; under hyperbaric conditions, however, the markedly raised arterial and choroidal PO₂ can supply enough oxygen by diffusion to keep the inner retina viable distal to the block - bridging the retina until spontaneous recanalisation or definitive measures restore flow.
Time is retina
Experimental and clinical data indicate a narrow therapeutic window - the best visual outcomes follow treatment started within hours of onset, before irreversible infarction. HBO is begun emergently and the patient kept oxygenated (continuing or repeating sessions guided by visual response) per a defined CRAO protocol. The retina is maintained on oxygen until it can tolerate room air without deterioration.
Role in management
- Treat as an emergency: do not delay HBO for non-essential investigations once CRAO is diagnosed.
- Exclude arteritic (giant-cell) aetiology - it mandates immediate corticosteroids and a different pathway.
- Mandatory parallel stroke work-up: CRAO carries a substantial early risk of cerebral stroke and myocardial infarction; activate the TIA/stroke pathway (carotid and cardiac evaluation).
Treatment approach
Treatment follows the unit's emergency CRAO protocol: prompt recompression on 100% oxygen, with pressure and session frequency titrated to the visual response and continued until the retina is stable off oxygen. Exact pressures and scheduling are individualised and set case by case.
Evidence base
The evidence is observational rather than randomised, but it has grown and now leans toward benefit. Two recent systematic reviews (Elfil 2025; ALBalawi 2026, 12 studies) found pooled visual-acuity improvement with HBO, with the largest gains when treatment starts within about 12 hours; an older, smaller meta-analysis (Rosignoli 2021) found no benefit. A prospective study using fluorescein angiography (Chiabo 2024) documented retinal re-perfusion in 87% of eyes by day 21, and the largest single cohort (Hadanny 2017, 128 patients) showed meaningful visual recovery - with an important practical lesson: the cherry-red spot on the retina, not the clock alone, marks the point of irreversibility.
A 2026 meta-analysis directly comparing HBO with intravenous thrombolysis (Bakdalieh) found the two give comparable visual gains (meaningful improvement in about 46% vs 42%), with similar overall complication rates but a safer profile for HBO (ear barotrauma versus the bleeding risks of thrombolysis). What remains unproven is HBO against no treatment at all - no randomised trial exists, and outcomes are limited by how quickly patients present. HBO is therefore a recognised UHMS indication delivered as a time-critical emergency within a multidisciplinary "eye-stroke" pathway.
Bottom line
Non-arteritic CRAO is an eye stroke: treat within hours, ideally under 12, and by the retinal appearance (before a cherry-red spot forms) rather than the clock alone. The observational evidence now leans positive and puts HBO at least on par with thrombolysis, with a safer profile - but it is not proven against no treatment, and it never replaces urgent stroke work-up or exclusion of giant-cell arteritis.
Talks & chapter reviews
Recorded talks, chapter reviews and the unit's CRAO protocol:
 UHMS Indications, Ch. 02a — Central Retinal Artery Occlusion
UHMS Indications, Ch. 02a — Central Retinal Artery Occlusion HMP, Ch. 32 — Central Retinal Artery Occlusion
HMP, Ch. 32 — Central Retinal Artery Occlusion CRAO 2025 — Extensive Overview
CRAO 2025 — Extensive Overview Stroke & MI Risk after Retinal Artery Occlusion
Stroke & MI Risk after Retinal Artery Occlusion HBOT for CRAO (overview)
HBOT for CRAO (overview)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Central Retinal Artery Occlusion.
- Mac Grory B, et al. Management of central retinal artery occlusion: a scientific statement from the American Heart Association. Stroke. 2021;52(6):e282-e294.
- ALBalawi HB, et al. Therapeutic efficacy of hyperbaric oxygen in central retinal artery occlusion: a systematic review and meta-analysis. J Clin Med. 2026;15(9):3530. doi:10.3390/jcm15093530
- Bakdalieh A, et al. Hyperbaric oxygen therapy versus intravenous thrombolysis in the treatment of central retinal artery occlusion: a systematic review and meta-analysis. J Clin Med. 2026;15(7):2628. doi:10.3390/jcm15072628
- Elfil M, et al. Hyperbaric oxygen therapy for central retinal artery occlusion: a systematic review and meta-analysis. Can J Neurol Sci. 2025. PMID 40739887.
- Chiabo J, et al. Efficacy and safety of hyperbaric oxygen therapy monitored by fluorescein angiography in patients with retinal artery occlusion. Br J Ophthalmol. 2024;108(7):956-62. doi:10.1136/bjo-2023-323972
- Hadanny A, et al. Reversibility of retinal ischemia due to central retinal artery occlusion by hyperbaric oxygen. Clin Ophthalmol. 2017;11:115-25. doi:10.2147/OPTH.S121307
The Eye Stroke: How High-Pressure Oxygen is Saving Sight in the 24-Hour Window
Introduction: the painless curtain
Imagine a sudden, painless curtain falling over the vision in one eye. There is no trauma, no warning, and no physical discomfort. This is the classic presentation of a central retinal artery occlusion (CRAO), a condition that for over a century was met with a grim medical shrug. Historically, prognosis was considered "hopeless and recalcitrant", with traditional treatments - such as ocular massage, paracentesis (draining fluid from the eye), or "carbogen" inhalation - failing to offer meaningful recovery. Today, however, an investigative look into clinical outcomes reveals a surprising hero: hyperbaric oxygen therapy (HBO2). What was once a permanent sentence of blindness is now a race against the clock, where oxygen serves as the primary drug for recovery.
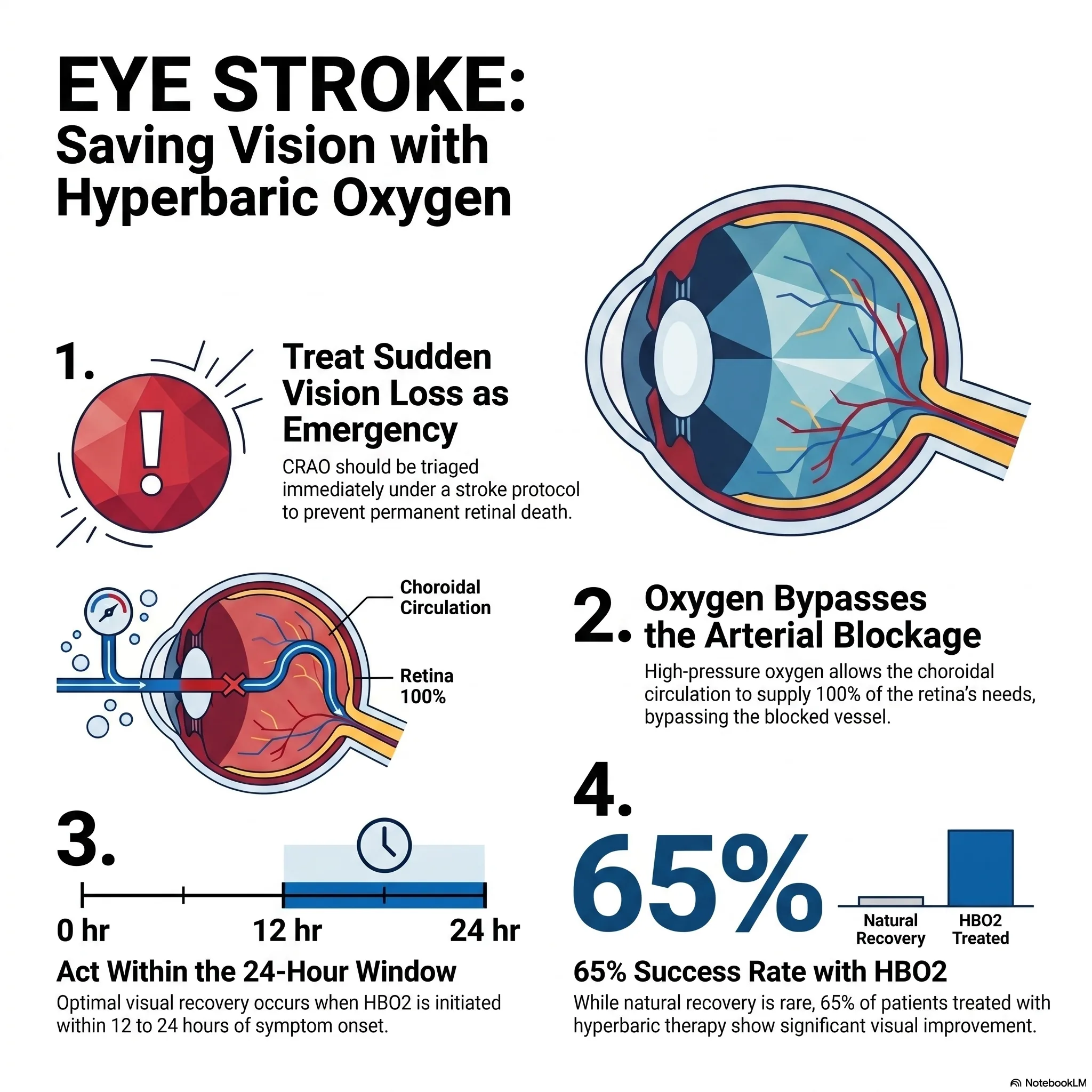
Takeaway 1: it's not just blindness, it's a stroke
Modern medicine is finally acknowledging a terrifying reality: CRAO is not an isolated eye problem; it is an emergency vascular event that belongs under a "stroke protocol." The retina and the brain share a common vascular origin, making the eye a literal window into the health of the cerebrovascular system. The data is striking: MRI screenings show that 32% of CRAO patients have incidental acute or subacute brain infarcts (mini-strokes) occurring simultaneously.
Furthermore, 78% of CRAO patients arrive at the emergency room with previously undiagnosed vascular risk factors, including critical carotid disease, hypertensive emergencies, or even active myocardial infarctions. Perhaps most telling of the systemic collapse involved is that 93% of hospitalised CRAO patients require an immediate change in their medications. As the clinical evidence suggests:
"MRI of CRAO patients found 32% had acute or subacute incidental brain infarcts, demonstrating the high-risk nature of these patients and need for admission from the emergency department."
Takeaway 2: the retina is the body's most oxygen-hungry organ
The retina is arguably the most metabolically demanding tissue in the human body, consuming oxygen at a rate of 13 mL per 100 grams of tissue every minute - a rate that exceeds even that of the brain. This extreme hunger makes the retina uniquely sensitive to ischaemia; when the blood supply is cut off, the clock doesn't just tick, it hammers.
When the central retinal artery is blocked, the tissue enters a state of "ischaemic penumbra." Clinicians often refer to this as the "idling retina" - tissue that is too weak to function (causing blindness) but is not yet dead. Borrowing from the cardiac mantra "time is muscle", health journalists and clinicians have a new rallying cry: "time is vision."
Takeaway 3: the "back door" strategy of hyperbaric oxygen
When the central retinal artery is occluded, the "front door" for oxygen is locked. However, the eye possesses a unique physiological "back door" known as the choroidal circulation. Under normal conditions, the choroid provides about 60% of the retina's oxygen.
Hyperbaric oxygen therapy works by using high pressure to dissolve massive amounts of oxygen directly into the blood plasma. This allows oxygen to diffuse from the choroid into the inner layers of the retina. This "bypass" is a physiological marvel: while the retinal vessels might constrict under high oxygen, the choroidal blood flow is notably unaffected by changes in oxygen tension. Under hyperbaric conditions, the choroid can provide 100% of the retina's required oxygen, keeping the "idling retina" alive until the blocked artery naturally recanalises - a process that typically takes up to 72 hours.
Takeaway 4: the 15% who have a "genetic safety net"
In the lottery of human anatomy, roughly 15% to 30% of the population carries a "genetic safety net" called the cilioretinal artery. This vessel is part of the ciliary arterial supply rather than the retinal system, yet it feeds the macula, the area responsible for sharp, central vision.
In these fortunate individuals, even a total occlusion of the main central retinal artery may spare their central vision. For the remaining 70% to 85% of the population, however, no such backup exists. For them, the only hope of preserving sight during a vascular blockage is the artificial "safety net" provided by a hyperbaric chamber.
Takeaway 5: the narrow 24-hour window of opportunity
While animal models (specifically rhesus monkeys) show permanent retinal damage in as little as 97 to 105 minutes, the human window is significantly wider. Clinical data supports treatment up to 24 hours after symptom onset. This discrepancy exists because, in humans, some "residual retinal blood flow" often remains, slowing the progression toward total cell death.
The urgency, however, cannot be overstated. While the overall success rate for HBO2 treatment is approximately 65%, that number jumps to a striking 82% when treatment is initiated within the first 8 hours. To catch this window, everyone should know the "red flags" that distinguish a vascular eye stroke from a mechanical issue:
- Sudden, painless loss of vision: often described as a "curtain" or profound blurring.
- Patient age over 40: CRAO is primarily a disease of the ageing vascular system; vision loss in younger patients often suggests alternate diagnoses.
- Lack of flashes or floaters: flashes often signal a mechanical "plumbing" issue like retinal detachment; their absence points to a vascular "flow" issue.
Takeaway 6: the economic paradox of vision
There is a profound economic paradox in how we treat "eye strokes." A full course of hyperbaric treatment typically costs between $2,000 and $5,000. When weighed against the lifelong cost of care, disability services, and lost productivity for a blind individual, the therapy is an undeniable bargain.
Yet an investigative look at the US healthcare landscape reveals a bottleneck: only 7% of US centres with both vascular neurology and retina programmes currently offer HBO2 for CRAO. This is a systemic failure. Despite being safe, efficacious, and potentially life-altering, the therapy remains underutilised in the very hospitals best equipped to provide it.
Conclusion: a call for urgent awareness
Central retinal artery occlusion is a medical emergency where oxygen is the difference between sight and permanent darkness. By using hyperbaric pressure to force oxygen through the eye's "back door", we can keep the retina viable until its natural circulation returns.
If untreated CRAO results in permanent blindness 80% of the time, yet early oxygen intervention offers upwards of an 82% success rate, we must confront a difficult question: why isn't this the universal standard of care? We must stop viewing the "eye stroke" as a localised tragedy and start treating it as the systemic emergency it is. In the battle for vision, every hour counts, and oxygen is the most powerful weapon we have.
This feature article is general educational information and does not replace advice from your own doctor or emergency services. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.