Hyperbaric Oxygen Therapy for Sudden Sensorineural Hearing Loss
Sudden deafness in one ear is an urgent problem. Hyperbaric oxygen - often combined with steroids - raises oxygen to the inner ear and can improve recovery when started early.
What this means for you
What is sudden sensorineural hearing loss?
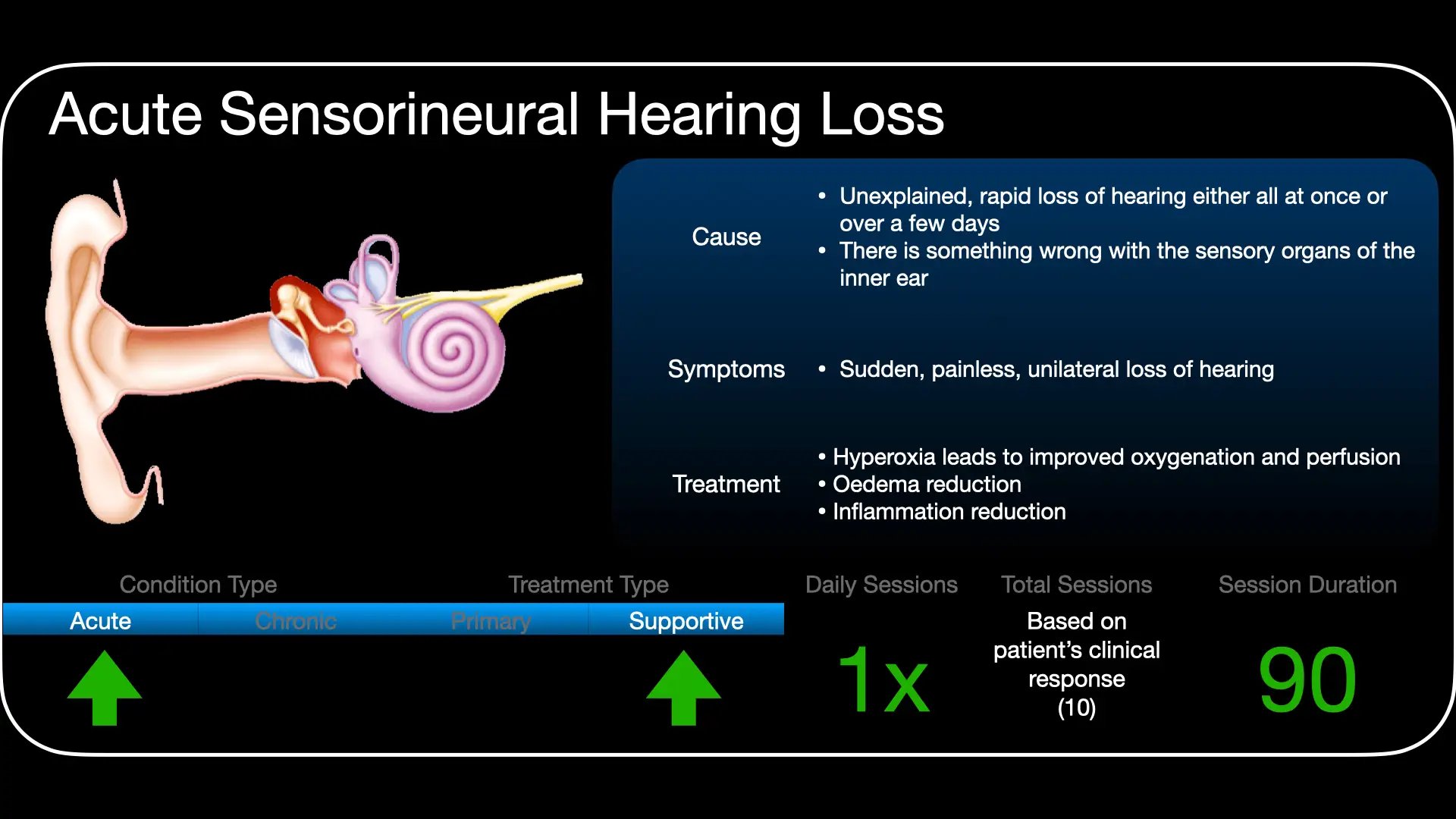
This is a rapid loss of hearing in one ear, coming on over a few hours to three days. It arises from the inner ear (the cochlea) or the hearing nerve, and often comes with ringing in the ear (tinnitus) or a blocked, full feeling. When no specific cause is found it is called idiopathic sudden sensorineural hearing loss. It can be frightening - and it needs prompt attention.
How can hyperbaric oxygen help?
The hearing organ inside the cochlea is one of the most oxygen-hungry tissues in the body, and its blood supply has little to fall back on. In sudden hearing loss the oxygen level in the inner ear drops. Breathing pure oxygen under pressure in the chamber raises that oxygen level dramatically, which can help the delicate hearing cells survive and recover. It is often used together with steroid treatment.
What to expect
When used, hyperbaric oxygen is given as a short course of regular sessions, alongside steroids and the care of your ENT team. Your hearing is tested before and during treatment to see how you respond. Whether it is suitable depends on how severe and how recent the loss is.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 A Sudden Silence (English)
A Sudden Silence (English) Skielike Gehoorverlies (Afrikaans)
Skielike Gehoorverlies (Afrikaans) For Patients: Sudden Hearing Loss (UHMS 09)
For Patients: Sudden Hearing Loss (UHMS 09)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
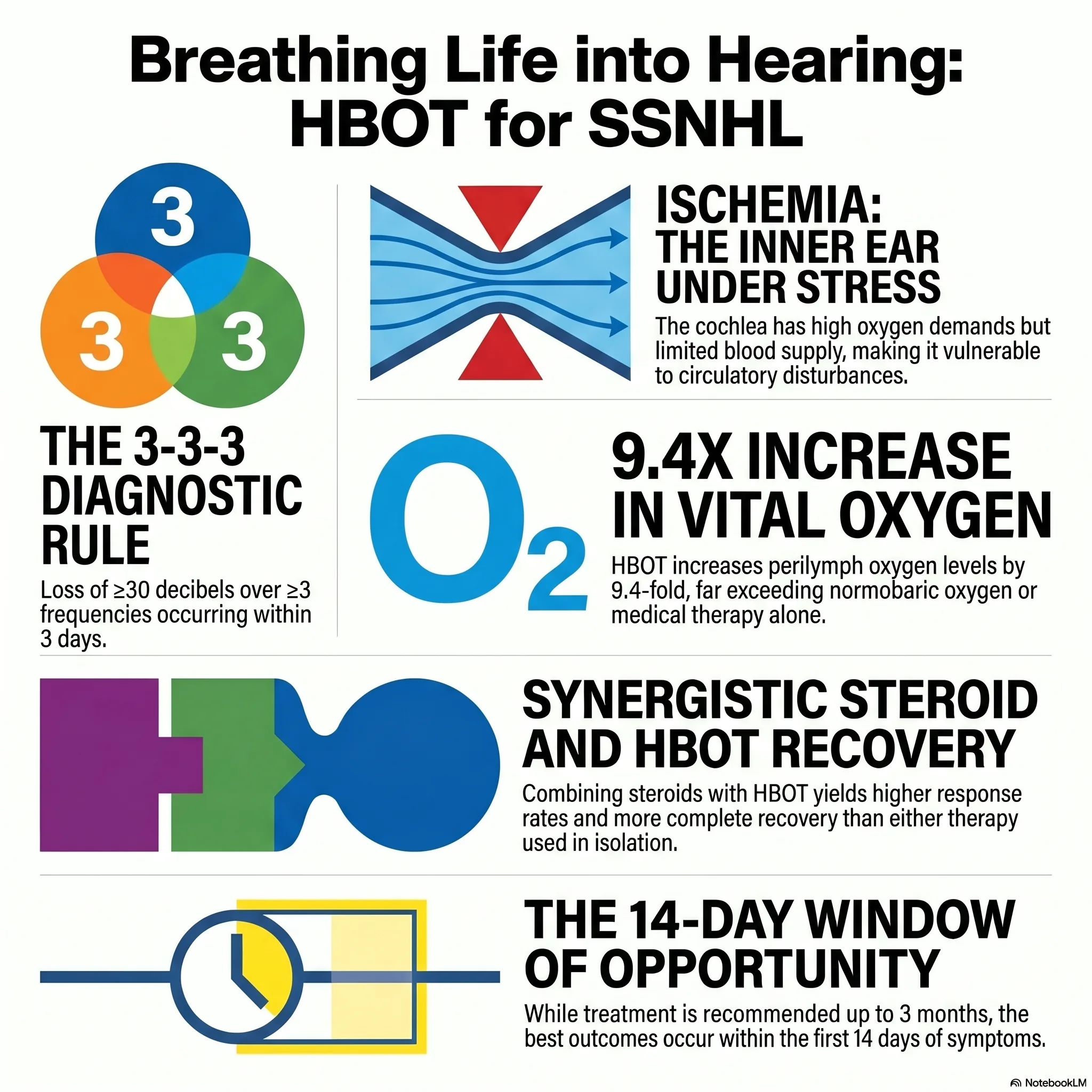
Idiopathic sudden sensorineural hearing loss (ISSNHL) is a recognised indication for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS), and is offered as an option in major otolaryngology guidance. It is typically defined as a sensorineural loss of ≥30 dB over ≥3 contiguous frequencies developing within 72 hours, with no identifiable cause.
Rationale
The cochlea has exceptionally high metabolic and oxygen demands and an end-arterial supply with negligible collateral. The organ of Corti is oxygenated largely by diffusion from the perilymph, whose oxygen tension falls in SSNHL. By markedly raising perilymph and cochlear oxygenation, HBO aims to support hair-cell survival and recovery during the critical early window.
Timing & selection
Benefit is strongly time-dependent: greatest when started within ~2 weeks of onset, declining thereafter (salvage may still be considered up to ~1-3 months, and up to 6 months for severe-to-profound loss). The largest gains are seen in severe-to-profound losses and when HBO is combined with corticosteroid therapy (systemic and/or intratympanic).
Role in management
- Refer early; do not delay - exclude retrocochlear pathology (MRI) and treat as urgent.
- HBO is used adjunctively with corticosteroids rather than as a stand-alone therapy in most protocols.
- Document audiometry before and during treatment to gauge response objectively.
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.5 ATA, daily, over a course typically in the order of 10-20 sessions, alongside corticosteroid therapy. Exact protocol is individualised and set case by case at the unit.
Evidence base
Several meta-analyses report better hearing recovery when HBO is added to standard steroid therapy. A large 2018 analysis (Rhee, 2,401 patients) found higher rates of complete and partial recovery with HBO, with the biggest gains in severe-to-profound loss, in salvage use, and with a longer total treatment dose. The most recent and largest reviews agree (Alter 2026; and the updated Cochrane review, Newth 2025), the latter finding a mean improvement of about 16 decibels and concluding that HBO plus steroids can be justified as a routine treatment when started within about 30 days of onset. HBO is a recognised UHMS indication and is offered as an option in the AAO-HNS clinical practice guideline.
We keep the framing honest. The trials pooled in these reviews are mostly small and of modest quality, the pooled evidence is graded moderate rather than strong, and at least one randomised trial found no significant benefit - so the effect is real but of uncertain everyday significance. Two consistent lessons hold across the evidence: treat early (the sooner the better, and the benefit fades with delay), and the greatest gains are in severe or profound loss and when HBO is used alongside steroids rather than instead of them. HBO is not used for chronic hearing loss or for tinnitus without acute hearing loss.
Bottom line
Sudden one-sided hearing loss is a medical urgency - see an ENT and start steroids promptly. Added early (ideally within days, and up to about 30 days), hyperbaric oxygen improves the chance of hearing recovery, most clearly in severe or profound loss and as a salvage option when steroids alone have not worked. It is an adjunct to steroid treatment, delivered over roughly 10-20 sessions, and progress is checked with repeat audiograms.
Talks & chapter reviews
Recorded talks, textbook-chapter reviews and case discussions on this indication:
 UHMS Indications, Ch. 09 — Sudden Sensorineural Hearing Loss
UHMS Indications, Ch. 09 — Sudden Sensorineural Hearing Loss HMP, Ch. 14 — Idiopathic SSNHL
HMP, Ch. 14 — Idiopathic SSNHL HBOT for Idiopathic SSNHL (overview)
HBOT for Idiopathic SSNHL (overview) Sudden Hearing Loss — case discussion
Sudden Hearing Loss — case discussionKey references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Idiopathic Sudden Sensorineural Hearing Loss.
- Newth A, Perleth M, Sherlock S, Romero L, Bennett MH. Hyperbaric oxygen therapy for acute idiopathic sudden sensorineural hearing loss; a systematic review with meta-analysis. Diving Hyperb Med. 2025;55(4):398-406. doi:10.28920/dhm55.4.398-406
- Alter IL, Hamiter M, Han J, et al. Hyperbaric oxygen and sudden sensorineural hearing loss: a systematic review and meta-analysis. Laryngoscope. 2026;136(1):91-101. doi:10.1002/lary.32472
- Rhee TM, Hwang D, Lee JS, et al. Addition of hyperbaric oxygen therapy vs medical therapy alone for idiopathic sudden sensorineural hearing loss: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2018;144(12):1153-61. doi:10.1001/jamaoto.2018.2133
- Joshua TG, et al. Hyperbaric oxygen therapy for patients with sudden sensorineural hearing loss: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2022. PMID 34709348.
- Chandrasekhar SS, et al. Clinical practice guideline: sudden hearing loss (update). Otolaryngol Head Neck Surg. 2019;161(1_suppl):S1-S45.
The Sound of Sudden Silence: Why Your Ear is the Body's Ultimate Warning System
Imagine waking up to a world that has suddenly gone quiet in one ear. You might assume it's a stubborn case of congestion or a simple wax buildup, but this "waking up" phenomenon is often the first sign of a high-stakes medical emergency: sudden sensorineural hearing loss (SSNHL).
While the medical community labels about 88% of these cases as "idiopathic" - meaning the cause is unknown - the clinical definition is precise. Idiopathic sudden sensorineural hearing loss (ISSHL) is characterised by a loss of at least 30 decibels across three contiguous frequencies, occurring within a seventy-two-hour window. This isn't just a localised "ear problem." Emerging research suggests that when the ear goes dark, it is acting as a "check engine light" for the body's most critical vascular and neurological systems.
Beyond the "rare" medical mystery
For decades, ISSHL was treated as a clinical rarity, with historical data suggesting only 5 to 20 cases per 100,000 people. However, that label is rapidly becoming outdated. Recent literature indicates that in the United States, the annual incidence is closer to 27 per 100,000, while international reports - specifically from Japan - have seen figures as high as 160 per 100,000.
The condition is particularly prevalent in the elderly, affecting 77 per 100,000, but it does not spare the young, with a paediatric incidence of 11 per 100,000. This upward trend in data reveals that ISSHL is a global health concern that demands immediate public awareness. If a patient or practitioner dismisses sudden silence as a minor ailment, they may be missing a critical window for systemic diagnosis.
The low blood pressure paradox
Conventional medical wisdom usually links vascular damage to hypertension (high blood pressure). However, a landmark study from the University of Bologna discovered a counter-intuitive link: systemic hypotension (low blood pressure) may be the primary culprit for young, otherwise healthy patients.
This finding challenges the traditional "clogged pipe" view that only high pressure and arterial "clogs" cause damage. To understand why this matters, one must look at the way the body prioritises blood flow. While the brain possesses robust circulatory autoregulation to protect itself during a blood pressure drop, the inner ear is significantly less "protected." It lacks the same autoregulatory strength, leaving it uniquely vulnerable to even minor dips in systemic pressure. This has immediate implications for treatment; historically, doctors might have reached for vasodilators to open up blood flow, but in a patient who is already hypotensive, these drugs could be dangerously counterproductive.
A warning sign for vascular catastrophe
One of the most sobering discoveries in recent years is the link between the inner ear and the brain's vascular integrity. In a study by Lin et al., researchers followed over 1,400 ISSHL patients for five years and found a 12.7% stroke rate, compared to just 8.7% in a control group.
What makes this study particularly compelling is the choice of the control group: patients admitted for appendicitis. While appendicitis is a sudden surgical event, it does not correlate with future vascular risk. Hearing loss, however, does. Statistically, ISSHL patients have a 1.64 times greater hazard of suffering a stroke within five years. Furthermore, an elevated neutrophil-lymphocyte ratio (NLR) in these patients can serve as a predictor for other ischaemic conditions, such as coronary or cerebral ischaemia. Essentially, the ear shares similar vascular vulnerabilities with the brain; a sudden "crash" in hearing is a systemic alarm that should prompt a high-priority follow-up with neurology or cardiology.
The inner ear's "oxygen hunger"
The structures within the inner ear, specifically the stria vascularis and the organ of Corti, are among the most metabolically active in the human body. They have a massive, constant demand for oxygen but rely on a minimal direct blood supply. This creates a state of perpetual "oxygen hunger."
When oxygen levels drop - a state known as hypoxic aetiology - the consequences are immediate and mechanical. The oxygen-dependent sodium and potassium pumps in the ear begin to fail, leading to intracellular sodium accumulation and microstructural damage. This results in the fusion and contraction of hair cell cilia and synaptic swelling.
This cellular "suffocation" is why hyperbaric oxygen therapy (HBO2) has become a cornerstone of recovery. While breathing normal air only slightly increases oxygen in the ear's fluids, HBO2 can increase perilymph oxygen concentrations by 9.4-fold. By flooding these hungry tissues with nearly ten times the normal oxygen level, clinicians can provide the fuel necessary for cellular repair and pump restoration.
The connection to spinal anaesthesia
The inner ear is not an isolated island; it is deeply connected to the body's pressure systems. This is most surprisingly illustrated in cases of hearing loss following non-cardiac surgeries, specifically those involving spinal anaesthesia.
When a needle puncture in the dura causes cerebrospinal fluid (CSF) volume and pressure to drop, that reduced pressure is transmitted directly to the inner ear via the cochlear aqueduct. This disrupts the delicate fluid balance between the endolymph and perilymph, essentially causing a pressure-induced "collapse" that damages sensitive hair cells. These cases serve as a vivid reminder that the body's pressure regulation is a full-body system; a procedure on the lower back can have a devastating impact on the ear.
The synergy of steroids and oxygen
While over 60 different protocols have been used to treat ISSHL, the combination of corticosteroids and hyperbaric oxygen therapy has emerged as the clear frontrunner. Corticosteroids work by reducing inflammation and oedema, calming the "cytokine storm" that can follow an ear insult. HBO2 then steps in to reverse the oxygen debt and restore cellular function.
The data supports this "dual-threat" approach. A 2015 study by Capuano showed that combination therapy resulted in an 84% response rate, significantly higher than using either treatment alone. Furthermore, HBO2 is the only treatment modality for ISSHL backed by a positive Cochrane Review, which calculated a "number needed to treat" (NNT) of 5.3 for a good outcome. In the world of medicine, an NNT of 5.3 is exceptional - it means for roughly every five people treated, one extra person achieves a significantly better outcome, a rate superior to many common interventions.
For patients who do not respond to initial oral or intravenous steroids, "salvage therapy" using intratympanic (IT) steroids - direct injections into the ear - has also shown promise in providing higher perilymph concentrations with fewer systemic side effects.
A 14-day "golden window"
Our understanding of sudden hearing loss has evolved from a simple "clogged pipe" theory to a complex, multifactorial understanding of vascular health and cellular metabolism. However, one clinical truth remains absolute: the importance of the "golden window."
While some guidelines suggest treatment can be attempted for up to three months, the most significant recovery happens when treatment begins within the first 14 days of symptom onset. If you or someone you know experiences a sudden drop in hearing, do not wait. The silence is not just a localised inconvenience; it may be your body's way of sending a high-priority signal about your total health. The question is: are you listening?
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.