Hyperbaric Oxygen Therapy for Avascular Necrosis
Avascular necrosis (osteonecrosis) is bone that dies when its blood supply is cut off - most often in the hip. In early stages, hyperbaric oxygen can raise the oxygen to the bone, ease the pressure inside it, and support repair.
What this means for you
What is avascular necrosis?
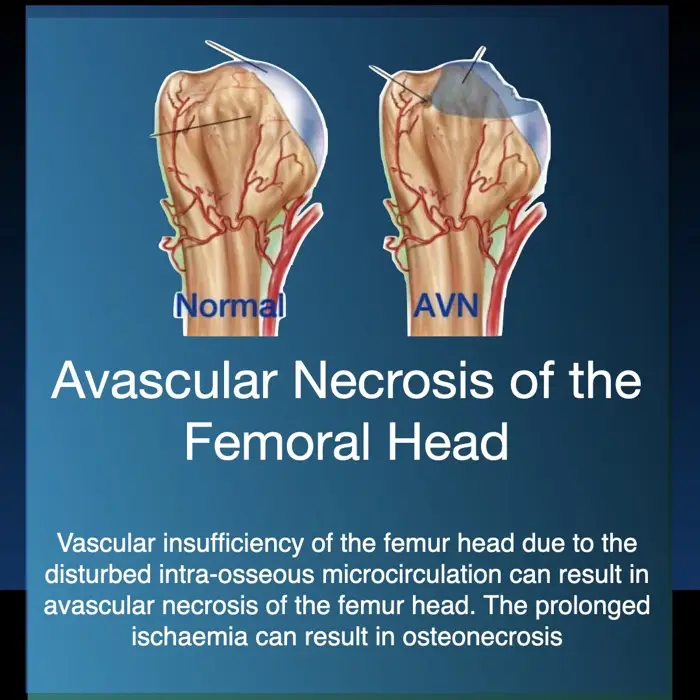
Bone is living tissue that needs a steady blood supply. In avascular necrosis - also called osteonecrosis - the blood supply to an area of bone is interrupted, and that piece of bone begins to die. It most commonly affects the head of the femur (the ball of the hip joint), but can occur elsewhere. Common contributors include previous injury, long-term steroid use, heavy alcohol use, and certain medical conditions.
Why does it matter?
Early on, avascular necrosis can be silent. As it progresses it causes joint pain and stiffness, and the weakened bone can eventually collapse, damaging the joint - which may then need a joint replacement. Picking it up and treating it early gives the best chance of protecting the joint.
How can hyperbaric oxygen help?
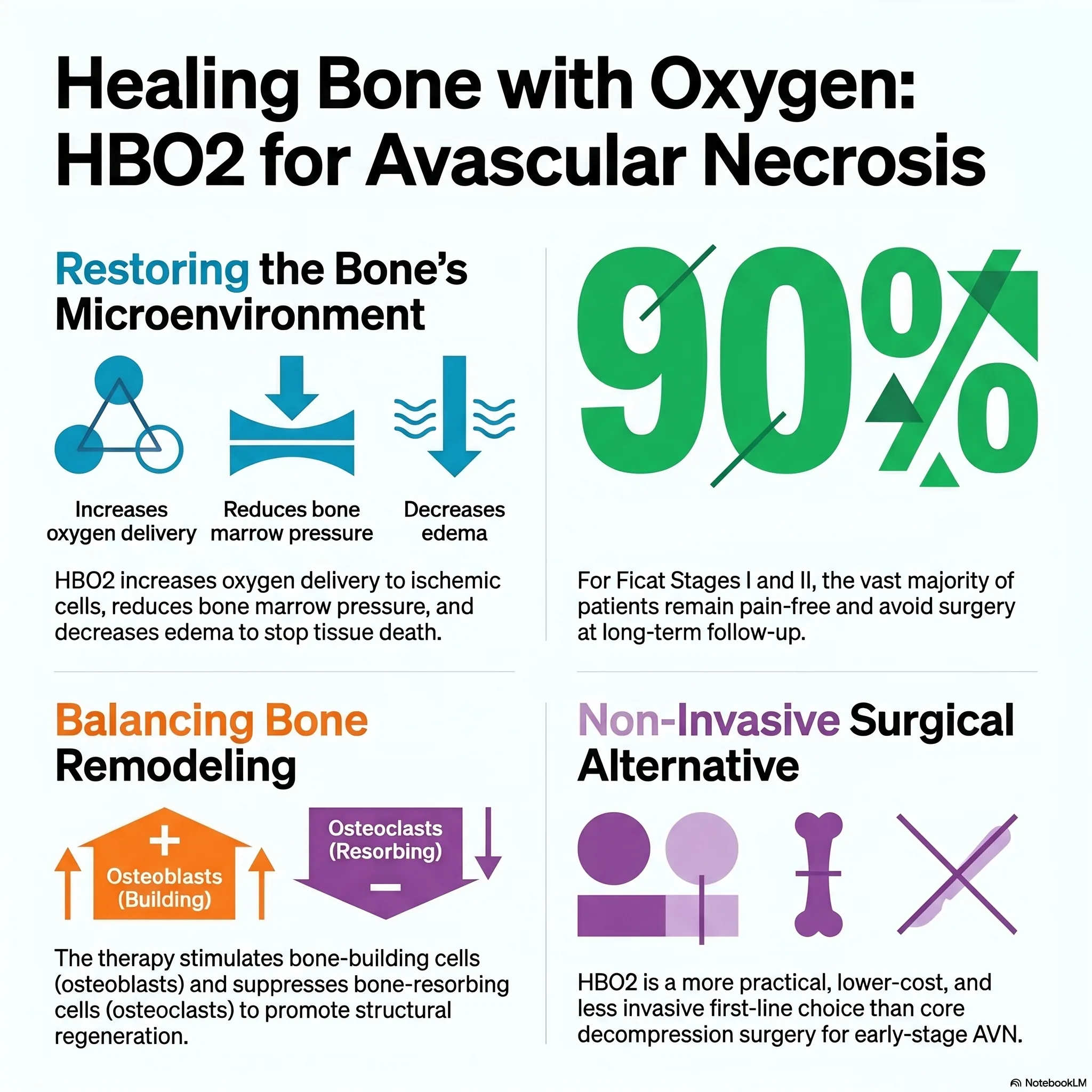
In the hyperbaric chamber you breathe pure oxygen under pressure, which raises the oxygen reaching the affected bone. This helps relieve the swelling and raised pressure that build up inside the bone, encourages new blood vessels to grow, and supports the bone's own repair. In the early stages - before the bone has collapsed - this can reduce pain and may slow the disease, potentially helping to delay or avoid a joint replacement.
What to expect
Treatment is given as a course of regular daily sessions over several weeks, with your progress followed - sometimes with repeat MRI scans. Whether it is suitable depends on the stage of the disease and your overall situation.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Avascular Necrosis & Hyperbaric Oxygen (English)
Avascular Necrosis & Hyperbaric Oxygen (English) 'n Been se Stille Dood (Afrikaans)
'n Been se Stille Dood (Afrikaans) For Patients: Avascular Necrosis (UHMS 15)
For Patients: Avascular Necrosis (UHMS 15)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Avascular necrosis (osteonecrosis), most commonly of the femoral head, is a recognised indication for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO is directed at early, pre-collapse disease (e.g. ARCO/Ficat stage I-II), where joint preservation is still achievable.
Pathophysiology
Interruption of the osseous blood supply produces marrow ischaemia, oedema and a rise in intraosseous pressure, establishing a self-perpetuating compartment-like cycle of hypoxia and impaired perfusion. Without intervention, subchondral fracture and articular collapse follow, leading to secondary osteoarthritis.
Mechanisms
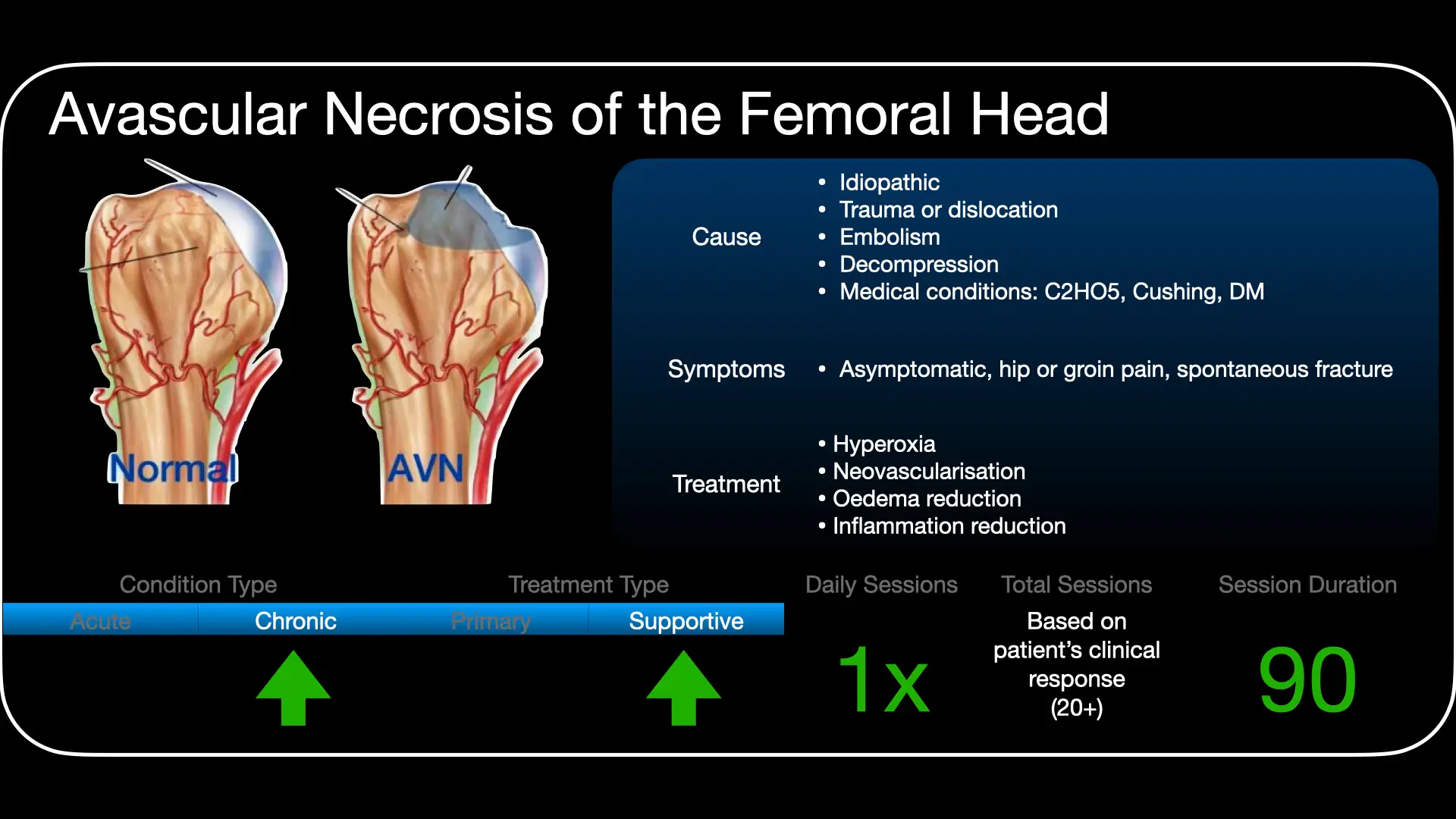
HBO raises oxygen tension in ischaemic marrow and, through hyperoxic vasoconstriction, reduces marrow oedema and intraosseous pressure - interrupting the ischaemia-oedema cycle. It promotes angiogenesis and revascularisation, supports osteoblast/osteoclast function and bone remodelling, and limits ischaemia-reperfusion injury. The result, in early disease, can be reduced pain, improved function, regression of marrow oedema on MRI and delayed progression.
Role in management
- Best results in early (pre-collapse) disease; benefit falls once subchondral collapse has occurred.
- Integrated with joint-preserving strategy - protected weight-bearing, risk-factor modification, and surgery (e.g. core decompression) where indicated.
- Stage with MRI; monitor response objectively (symptoms, function, imaging).
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.5 ATA, daily, over an extended course (often in the order of 20-30+ sessions, sometimes more), individualised to stage and response. Exact protocol is set case by case at the unit.
Evidence base
Avascular necrosis of the femoral head is an accepted hyperbaric indication in the UHMS 15th-edition Indications Manual (2023, Chapter 15), which endorses HBO for early (pre-collapse) disease at a 2B evidence grade, and in the European (ECHM) consensus at Type 2 / Level B. A double-blind randomised trial in Ficat stage II disease (Camporesi 2010) reported better pain and range of motion and, at seven years, joint preservation with no hip replacement; a comparative cohort in even earlier (stage I) disease showed MRI normalisation in most treated hips. Two meta-analyses (Li 2017; Paderno 2021) pooled a positive clinical effect.
We present the evidence honestly, because it is mixed. The most recent meta-analysis (Cao 2025) found that although patients improve after HBO, the improvement was not significantly greater than in patients who did not receive it, concluding HBO "cannot be regarded as an effective measure" for early femoral-head necrosis - and no trial has yet proven HBO against no treatment. The positive trials and the UHMS chapter also share authorship, which we note for balance. HBO is therefore offered as a selective, early-stage, joint-preserving adjunct - never as an isolated treatment.
Bottom line
HBO is a recognised option (UHMS 15th ed; ECHM) for early, pre-collapse femoral-head necrosis, aiming to relieve pain and preserve the joint before collapse. It is used alongside offloading (crutches), weight reduction and smoking cessation, and monitored by MRI - not as a substitute for surgery, which should not be delayed once the femoral head has collapsed. The evidence supports a trial in early disease but does not prove benefit over no treatment; response is assessed objectively and treatment stopped if the joint is not responding.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 15 — Avascular Necrosis
UHMS Indications, Ch. 15 — Avascular Necrosis HMP, Ch. 34 — HBO for AVN of the Femoral Head
HMP, Ch. 34 — HBO for AVN of the Femoral Head HBOT for AVN of the Femoral Head (SAUHMA)
HBOT for AVN of the Femoral Head (SAUHMA) UHMS — HBO for Avascular Necrosis (overview)
UHMS — HBO for Avascular Necrosis (overview)Key references
- Camporesi EM, Zanon V, Vezzani G, Bosco G. Avascular Necrosis (Aseptic Osteonecrosis). In: Hyperbaric Oxygen Therapy Indications, 15th ed. Undersea & Hyperbaric Medical Society; 2023. Chapter 15.
- Camporesi EM, Vezzani G, Bosco G, et al. Hyperbaric oxygen therapy in femoral head necrosis. J Arthroplasty. 2010;25(6 Suppl):118-23. PMID 20637561.
- Li W, Ye Z, Wang W, et al. Clinical effect of hyperbaric oxygen therapy in the treatment of femoral head necrosis: a systematic review and meta-analysis. Orthopade. 2017;46(5):440-6. doi:10.1007/s00132-016-3360-8
- Paderno E, Zanon V, Vezzani G, et al. Evidence-supported HBO therapy in femoral head necrosis: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(6):2888. doi:10.3390/ijerph18062888
- Cao Y, Tang P, Tan H, et al. Application of hyperbaric oxygen therapy in femoral head necrosis: a systematic review and meta-analysis. EFORT Open Rev. 2025;10(7):466-74. doi:10.1530/EOR-2024-0167
- Mathieu D, Marroni A, Kot J. Tenth European Consensus Conference on Hyperbaric Medicine: recommendations for accepted and non-accepted clinical indications. Diving Hyperb Med. 2017;47(1):24-32. doi:10.28920/dhm47.1.24-32
Saving Bone Without Surgery: The Surprising Power of Hyperbaric Oxygen for AVN
1. Introduction: the "silent" bone crisis
Avascular necrosis (AVN) is a medical term that masks a brutal reality: your bone tissue is literally dying. Also known as aseptic osteonecrosis, the condition is triggered by a localised "blackout" of blood flow, usually to the terminal vascular beds of the bone. Deprived of oxygen and nutrients, the cellular architecture of the bone begins to collapse, leading to a structural failure that can turn a healthy joint into a site of excruciating, permanent damage.
The stakes are particularly high because AVN doesn't discriminate based on age. It frequently strikes active adults between 40 and 50 - individuals in the prime of their professional and personal lives. Traditionally, the clinical path has been narrow and daunting, usually ending in total hip arthroplasty (THA), or a complete joint replacement. However, a non-invasive technology is rewriting this prognosis. Hyperbaric oxygen therapy (HBO2) is emerging as a surprising and powerful alternative, offering a way to save the bone before the surgeon's knife becomes the only option.
Takeaway 1: the 81% success rate vs. the 17% standard
In the world of orthopaedic medicine, "success" is defined by two factors: staying pain-free and avoiding the operating table. When we compare long-term outcomes, the data in favour of hyperbaric intervention is striking.
While traditional conservative management often fails to stop the progression of the disease, oxygen under pressure fundamentally alters the trajectory. Research comparing HBO2 against standard control groups reveals a massive gap in joint preservation over time. Hyperbaric oxygen has been documented to have a success rate of 81% at the seven-year follow-up, compared to only 17% for patients in the control group.
This isn't just a temporary delay; it represents a durable, seven-year clinical victory for the vast majority of patients treated with oxygen.
Takeaway 2: why "Stage I and II" are the golden window
The timing of the intervention is the single most critical factor for success. Orthopaedists use the Ficat classification system to stage the disease, and understanding where you fall on this scale is vital.
- Stage I: characterised by pain, but radiographs (X-rays) still appear normal.
- Stage II: the first signs of trouble appear on imaging, showing increased bone density, cystic changes, or porosity.
These early stages represent a "golden window." According to the Vezzani retrospective study, approximately 90% of patients in Ficat Stages I and II achieved complete recovery - meaning they remained pain-free and avoided surgery for at least a four-year follow-up period. Because Stage I is invisible to X-rays, the MRI remains the "gold standard" for catching AVN early enough to allow for a non-surgical save.
Takeaway 3: it's not just for hips
While the femoral head (the hip) is the most frequent victim of necrosis, AVN can strike almost any "osseous district" in the body. HBO2 has shown remarkable efficacy across various anatomical sites where blood flow has been compromised. According to clinical data from a variety of orthopaedic cases, high-pressure oxygen therapy provides significant relief in areas including:
- Femoral condyles (knee): 63.9% of patients reported no residual symptoms post-treatment.
- Humeral head (shoulder): 54.6% of cases achieved a state of no residual symptoms.
- The talus, tarsus, and calcaneus (ankle and heel): these complex, weight-bearing structures of the foot respond favourably to hyperbaric pressure.
Takeaway 4: shifting the cellular balance (the OPG/RANKL factor)
The real magic of HBO2 happens at the cellular level, where it acts as a biological "reset button" for bone remodelling. Your body constantly balances osteoblasts (bone-builders) and osteoclasts (bone-destroyers). AVN tilts this balance toward destruction.
HBO2 shifts the balance back by increasing serum concentrations of osteoprotegerin (OPG), a protein that suppresses the activation of bone-destroying osteoclasts. Simultaneously, the therapy accelerates the differentiation of bone-forming osteoblasts.
The physics of the treatment are just as important as the biology. To achieve these results, patients typically undergo 30-session cycles at 2.5 ATA (atmospheres absolute) for 90 minutes of 100% inspired oxygen. This high-pressure environment induces vasoconstriction, which sounds counter-intuitive but is actually the key to relief. By narrowing the blood vessels, HBO2 reduces oedema (swelling) within the rigid confines of the bone. This reduction in swelling effectively "relieves the compartment syndrome" inside the bone, lowering internal pressure and restoring life-giving oxygen to ischaemic cells.
Takeaway 5: avoiding the "bisphosphonate paradox"
For years, the standard pharmaceutical approach to AVN has included analgesics, vasodilators, and bisphosphonates. However, these medications come with a dark irony.
While bisphosphonates are prescribed to stop bone death in the hip, they are themselves a known cause of bisphosphonate-related osteonecrosis of the jaw (BRONJ). It is a medical paradox: a drug meant to save your hip can cause the bone in your jaw to die and expose itself through the gums. HBO2 offers a safer, cleaner alternative. It can also be used synergistically with surgical procedures like core decompression (CD) - a procedure that creates a channel in the bone to reduce pressure - to enhance healing in more advanced cases without the risks inherent in bone-altering medications.
Takeaway 6: "buying time" for younger patients
When a patient reaches Ficat Stage III, the bone has begun to flatten (the "crescent sign") and collapse is imminent. In these cases, the clinical goal shifts from total recovery to "buying time."
For a patient in their 30s or 40s, this is a vital strategy. Total joint replacements have a finite lifespan; every year a patient can keep their natural joint is a year they won't spend in a future revision surgery. For particularly young patients, the use of non-operative methods like HBO2 can "buy time" to minimise the total number of possible THA operations and subsequent revisions over a lifetime.
This is especially critical for paediatric and adolescent populations, such as those suffering from necrosis as a side effect of chemotherapy, where joint preservation is the primary clinical priority.
Conclusion: a new breath for orthopaedics
We are witnessing a fundamental shift in how we treat "inevitable" bone decay. By utilising hyperbaric oxygen to facilitate the oxygenation of hypoxic tissue and modulate the body's internal bone-remodelling system, we are moving away from a world where surgery is the only answer.
As we look toward the future of "oxygen as medicine", we must ask: if we can regrow bone and reverse necrosis with nothing more than air and pressure, what other surgical "certainties" might we eventually outpace? For now, the most important takeaway is simple: persistent joint pain with no clear injury demands an early MRI. Catching AVN in its silent, early stages is the difference between a lifetime of prosthetic revisions and a successful, non-surgical recovery.
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.