Hyperbaric Oxygen Therapy for Intracranial Abscess
An intracranial (brain) abscess is a pocket of pus inside the skull. Hyperbaric oxygen is used as an adjunct - especially for multiple or surgically inaccessible abscesses - alongside surgery and antibiotics.
What this means for you
What is an intracranial abscess?
An intracranial abscess is a collection of pus that forms inside the skull - in the brain itself or in its coverings. It usually develops when an infection spreads from the ears, sinuses or teeth, travels in the bloodstream, or follows a head injury or operation. Because it sits in an enclosed space, it can press on the brain, so it always needs urgent specialist care.
How is it usually treated?
The main treatments are a neurosurgical procedure to drain the pus and a prolonged course of antibiotics, with close monitoring. In certain situations - for example when there are several abscesses, when one is in a place that is difficult or risky to reach surgically, or when someone is too unwell for surgery or has a weakened immune system - hyperbaric oxygen can be added.
How can hyperbaric oxygen help?
In the chamber you breathe pure oxygen under pressure, which raises the oxygen reaching the infected, oxygen-poor area. Many of the bacteria that cause brain abscesses dislike oxygen, so this can help slow them, while also supporting the body's infection-fighting cells and helping to settle swelling around the abscess. It is used together with drainage and antibiotics, not instead of them.
What to expect
When used, hyperbaric oxygen is given as regular sessions over a period decided by the team, coordinated with your neurosurgical and infectious-disease care. Whether it is suitable depends on your scans, the type of infection and your overall condition.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Oxygen vs Brain Infections (English)
Oxygen vs Brain Infections (English) Brein Onder Beleg (Afrikaans)
Brein Onder Beleg (Afrikaans) For Patients: Intracranial Abscess (UHMS 10)
For Patients: Intracranial Abscess (UHMS 10)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Intracranial abscess - cerebral abscess, subdural empyema and intracranial epidural abscess - is a recognised indication for adjunctive hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO complements neurosurgical drainage and prolonged antimicrobial therapy and is particularly considered in defined high-risk scenarios.
When to consider HBO
- Multiple abscesses, or abscess in a deep / dominant / surgically inaccessible location.
- Patient at high surgical/anaesthetic risk, or immunocompromised host.
- Poor or slow response to standard surgical and antimicrobial therapy, or recurrence.
Mechanisms
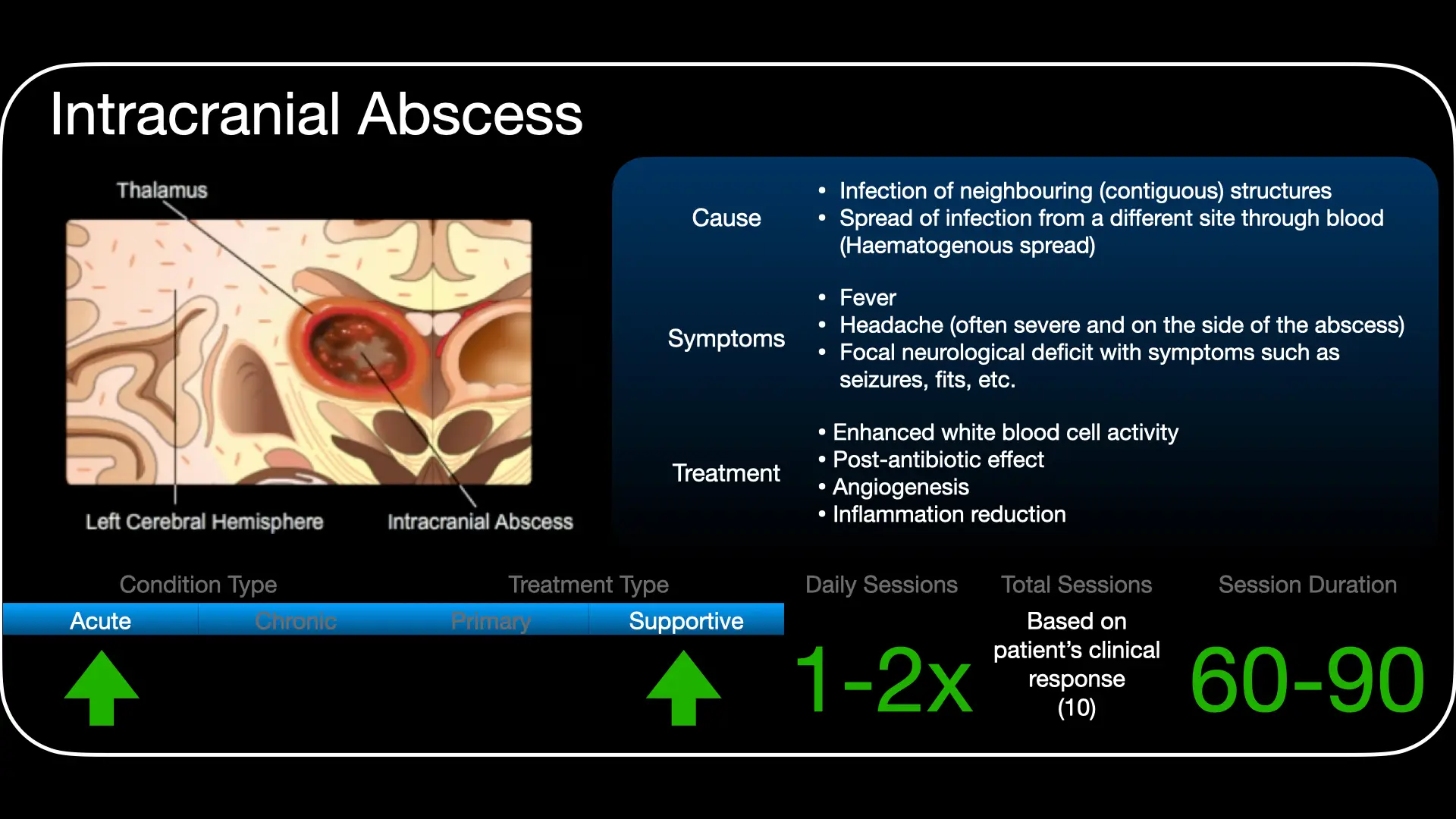
The abscess interior is hypoxic and favours anaerobes. HBO raises oxygen tensions in and around the lesion, which is directly inhibitory to anaerobic organisms, restores oxygen-dependent leukocyte bactericidal activity, promotes capsule formation and demarcation, and helps reduce surrounding cerebral oedema and intracranial pressure. These effects support the host while drainage and antibiotics address the source.
Role in management
HBO is an adjunct, not a substitute for source control: aspiration/excision where feasible and culture-directed antibiotics remain central. It is integrated with neurosurgical and infectious-disease care, with imaging follow-up to track response.
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.5 ATA, usually once daily over a course guided by clinical and radiological response. Exact protocol and duration are individualised and set case by case at the unit.
Evidence base
Because a brain abscess is life-threatening, a randomised trial is neither practical nor ethical, so the evidence is a strong biological rationale plus consistent clinical experience. A controlled study (Bartek 2016, 40 patients) reported that adding HBO led to fewer repeat operations (10% vs 45%) and better long-term recovery (good outcome in 80% vs 45%), and published case series report low complication rates. The governing hyperbaric review (Tomoye & Moon 2021) concludes that, given the high mortality of these infections and HBO's low risk, the risk-benefit balance favours adding HBO in selected patients. It is a recognised UHMS indication, carried in the 15th-edition Indications Manual.
Bottom line
Surgical drainage and a long course of intravenous antibiotics remain the primary treatment. Added afterwards, hyperbaric oxygen restores the oxygen-dependent bacteria-killing that neutrophils and antibiotics need in the hypoxic abscess, suppresses anaerobic organisms, and reduces surrounding brain swelling. It is most valuable when there are multiple abscesses, a surgically inaccessible or deep location, a poor surgical candidate, or a failure to respond to surgery and antibiotics alone - always as an adjunct, never a substitute for drainage.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 10 — Intracranial Abscess
UHMS Indications, Ch. 10 — Intracranial Abscess HMP, Ch. 19 — HBO in Intracranial Abscess
HMP, Ch. 19 — HBO in Intracranial Abscess HBOT for Intracranial Abscess (overview)
HBOT for Intracranial Abscess (overview) HBOT for Surgically Inaccessible Brain Abscesses
HBOT for Surgically Inaccessible Brain AbscessesKey references
- Tomoye EO, Park CL, Folke L, Moon RE. Intracranial Abscess. In: Hyperbaric Oxygen Therapy Indications, 15th ed (2023). Undersea & Hyperbaric Medical Society. (Reprinted: Undersea Hyperb Med. 2024;51(4):449-55. PMID 39821772.)
- Tomoye EO, Moon RE. Hyperbaric oxygen for intracranial abscess. Undersea Hyperb Med. 2021;48(1):97-102. doi:10.22462/01.03.2021.12
- Bartek J Jr, et al. Hyperbaric oxygen therapy in spontaneous brain abscess patients: a population-based comparative cohort study. Acta Neurochir (Wien). 2016. PMID 27113742.
- Kutlay M, et al. Stereotactic aspiration and antibiotic treatment combined with hyperbaric oxygen therapy in the management of bacterial brain abscesses. Neurosurgery. 2008.
The Surprising Science of Using Oxygen to Fight Brain Infections
An intracranial abscess (ICA) is a medical emergency that often begins in the shadows of the mundane. Whether manifesting as a cerebral abscess, a subdural empyema, or an epidural empyema, an ICA represents a collection of infected material within the skull - a literal "hidden emergency" that can arise from a simple sinus headache or a neglected dental infection. Yet the reach of this invader is broader than mere hygiene; it strikes children with cyanotic congenital heart disease and appears as a devastating complication of intravenous drug use.
While the incidence is relatively low - affecting between 0.4 and 0.9 people per 100,000 in the United States annually - the stakes are absolute. In 1960, an ICA was frequently a death sentence, with mortality rates hovering around 40%. Today, thanks to refined imaging and minimally invasive surgery, that number has plummeted to 10%. However, for those in the "refractory" category - where standard drugs and surgeries fail - the pressure is on to find a more effective solution.
The mouth-brain connection: a counter-intuitive culprit
To understand how to fight these infections, we must first look at where they come from. Investigative data reveals a surprising truth: many brain abscesses are caused by the "normal residents" of the human body. Between 30% and 50% of cases occur due to "contiguous spread", where bacteria from a nearby site - such as the sinuses or ears - migrate into the brain.
The primary culprits are often bacteria from the Viridans group, specifically Streptococcus intermedius, S. constellatus, and S. anginosus. While we might expect these in the oral cavity, they are also standard inhabitants of the appendix and the female genital tract. They possess a unique "proclivity for abscess formation" once they breach the blood-brain barrier.
"The aforementioned organisms [Streptococcus intermedius, constellatus, and anginosus] are distinct from Streptococcus pyogenes and Streptococcus pneumoniae, which are rare causes of bacterial brain abscess."
This distinction is vital for clinical investigative work. These organisms are not the common triggers for strep throat or pneumonia; they are specialised invaders that thrive in the unique, low-oxygen niches of the cranium.
The low-oxygen trap: why fungal infections are deadly
While bacteria are the primary suspects, fungal infections like Aspergillus or those from the Mucorales family represent a lethal subset of ICAs. These fungi are "angioinvasive", meaning they attack and block blood vessels, causing thrombophlebitis. This leads to local tissue death (necrosis) and creates a biological "catch-22".
This process results in a low-oxygen environment characterised by metabolic acidosis. In this acidic, oxygen-starved state, the body's primary defenders - neutrophils and macrophages - become paralysed. They require oxygen to perform the "respiratory burst" necessary to kill pathogens. By destroying the local blood supply, the infection effectively builds a fortress that keeps the immune system out, rendering traditional treatments nearly useless in these necrotic "dead zones".
Takeaway 1: HBO2 is an antibiotic force multiplier
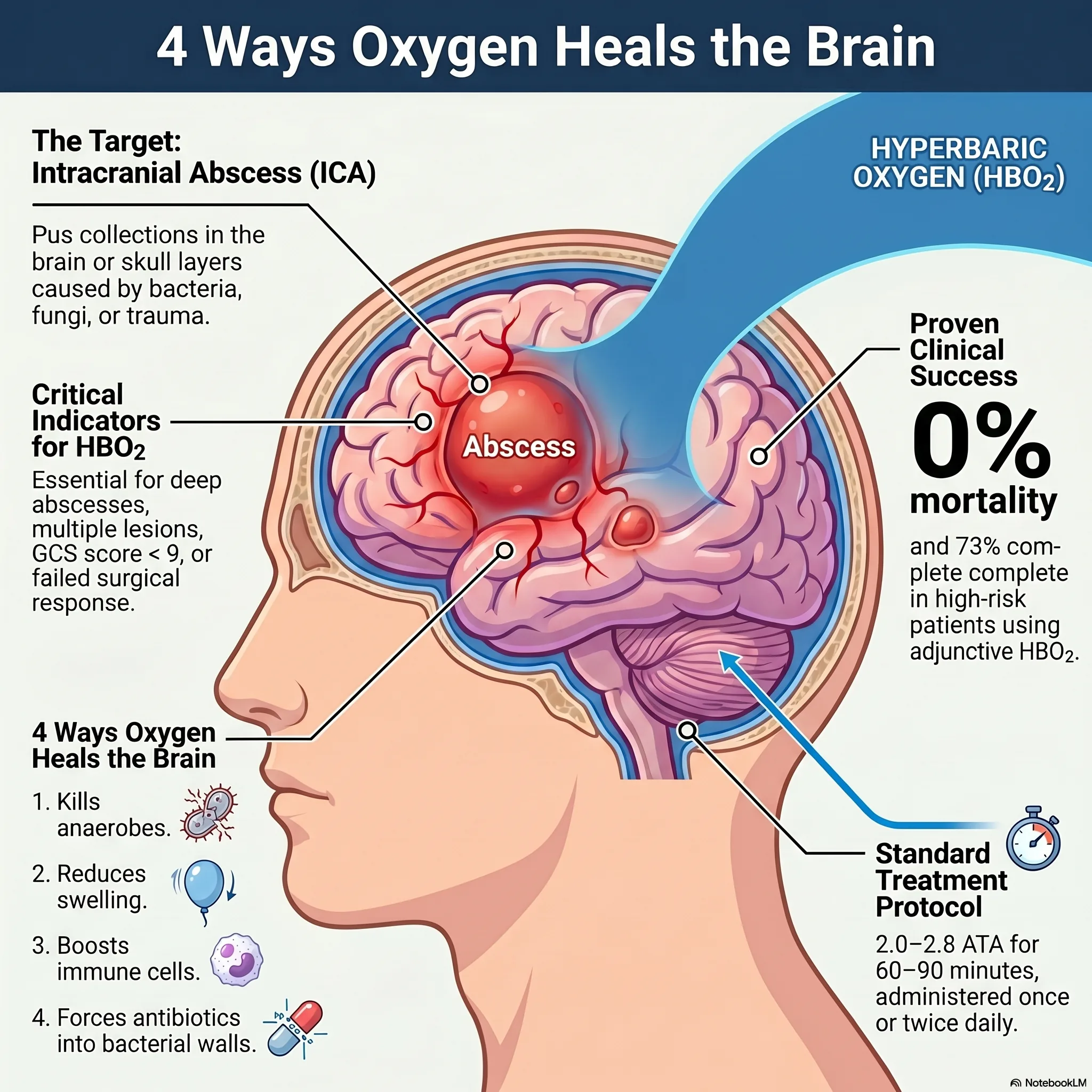
Hyperbaric oxygen therapy (HBO2) is more than a passive supplement; it is a restorer of pharmacological function. The active transport of critical antibiotics, such as cephalosporins and aminoglycosides, across bacterial cell walls is an oxygen-dependent process. When tissue oxygen (PO2) levels drop below the threshold of 20-30 mmHg - a common occurrence in abscessed tissue - this transport mechanism fails. HBO2 raises these levels, effectively "restarting" the antibiotics' ability to penetrate the bacteria.
Takeaway 2: fighting swelling without steroids
HBO2 provides a mechanical advantage by reducing perifocal brain swelling (oedema) through hyperoxic vasoconstriction. This is a major clinical advantage because it allows doctors to manage intracranial pressure without high-dose steroids. While steroids reduce swelling, they can also inadvertently impair the penetration of anti-infective medications across the blood-brain barrier, potentially shielding the infection from the very drugs meant to kill it.
The "refractory" criteria: when pressure becomes the last resort
HBO2 is not a first-line treatment for every patient, but it becomes a vital adjunct when the clinical picture darkens. According to established treatment flowcharts, HBO2 should be strongly considered when a patient presents with predictors of poor outcome or fails to respond to initial care. The specific criteria include:
- Multiple abscesses or those in a deep or dominant location: targeting areas that control speech or motor skills where surgery is high-risk.
- Glasgow Coma Scale (GCS) score less than nine: indicating severe neurological compromise.
- Compromised host: particularly those with HIV, malignancy, or diabetes (who are prone to rhinocerebral mucormycosis).
- Failure to respond: continued deterioration despite targeted antibiotics and standard surgical interventions (such as one or two needle aspirations).
Success in extremis: from infants to teens
The clinical evidence for HBO2 is growing through impactful series and case reports. One study of 25 consecutive patients treated with adjunctive HBO2 reported a 0% mortality rate, with 73% of patients achieving a complete recovery. Recent cases illustrate the therapy's power in desperate scenarios:
- Rhino-orbital-cerebral mucormycosis (ROCM): a 2021 series successfully used HBO2 to treat this aggressive fungal infection, which typically thrives in the acidic environments of diabetic patients. Six out of seven patients in the study showed complete resolution after 40-60 treatments.
- The 16-year-old recovery: a previously healthy teenager with multiple abscesses caused by Fusobacterium failed to improve after four surgeries. After initiating HBO2 at 2.8 ATA, he showed significant improvement after the first treatment and made a full recovery after 37 sessions.
- The 8-month-old infant: HBO2 was successfully utilised to treat a posterior fossa epidural abscess, proving the therapy's safety and efficacy even in paediatric patients.
Conclusion: the future of high-pressure healing
The battle against intracranial abscesses has transitioned from a 40% mortality rate in 1960 to a 10% rate today. This progress is a triumph of modern medicine, yet for the most difficult, "unreachable" infections, HBO2 remains an essential tool. By reversing metabolic acidosis and re-oxygenating necrotic tissue, HBO2 breaks the cycle of immune failure.
As we look forward, the success of oxygen in the brain suggests a broader potential. If hyperbaric pressure can solve an infection hidden deep within the cranium or lingering in the bone of the skull (as seen in concomitant skull osteomyelitis), could it be the key to solving other "unreachable" or antibiotic-resistant infections throughout the body? For patients under the most extreme pressure, high-pressure oxygen is proving to be more than just a breath of air - it is a lifeline.
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.