Hyperbaric Oxygen Therapy for Gas Gangrene
Gas gangrene (clostridial myonecrosis) is a rare, fast-moving muscle infection and a true emergency. Hyperbaric oxygen works alongside urgent surgery and antibiotics to help stop the bacteria in their tracks.
What this means for you
What is gas gangrene?
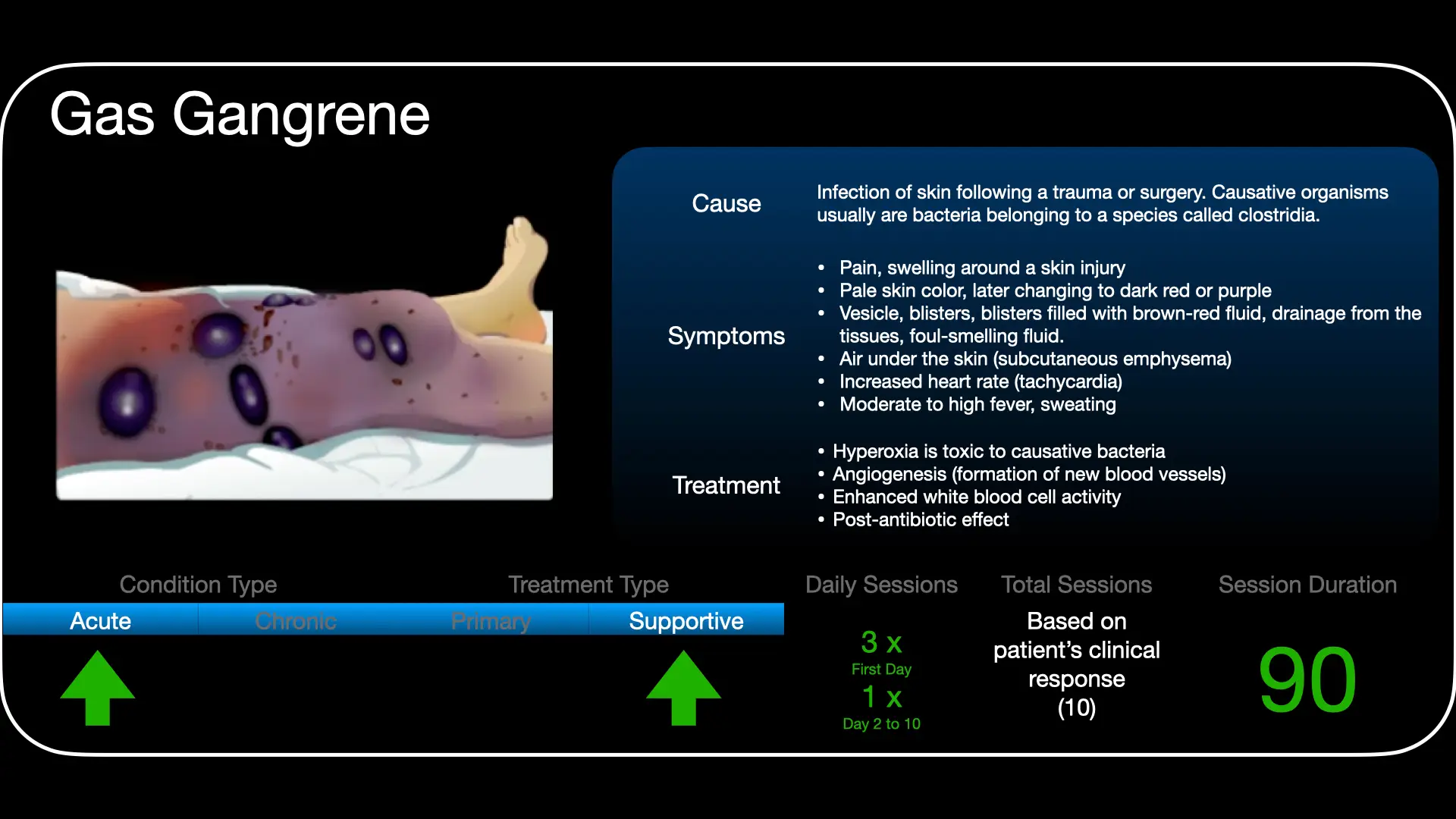
Gas gangrene, or clostridial myonecrosis, is a rare but very serious infection of the muscle. It is caused by Clostridium bacteria that grow where there is little oxygen - typically in a deep, dirty, or crush wound. These bacteria multiply quickly, release a powerful toxin that destroys muscle, and produce gas that can be felt as a crackling under the skin.
Why is it so dangerous?
The infection can spread within hours and make a person extremely ill, so it is treated as an emergency. Early signs include severe pain that seems out of proportion to the wound, swelling, discoloured skin, and a feeling of being very unwell.
How can hyperbaric oxygen help?
Hyperbaric oxygen therapy is used together with surgery and antibiotics - not instead of them. In the chamber you breathe pure oxygen under pressure, which drives a large amount of oxygen into the infected tissue. Because these bacteria cannot survive in an oxygen-rich environment, this helps stop them multiplying, switches off the toxin they produce, and supports your body's own infection-fighting cells. This can help limit how much tissue is lost.
What to expect
When hyperbaric oxygen is used for this condition it is given urgently and often several times in the first day or two, fitted around your surgery and intensive-care treatment. The exact schedule is decided by the team for your situation.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 Gas Gangrene: The Blitzkrieg (English)
Gas Gangrene: The Blitzkrieg (English) Gasgangreen - 'n Bio-Blitz (Afrikaans)
Gasgangreen - 'n Bio-Blitz (Afrikaans) For Patients: Clostridial Myonecrosis (UHMS 04)
For Patients: Clostridial Myonecrosis (UHMS 04)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Clostridial myonecrosis (gas gangrene) is a recognised indication for hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO is an adjunct to the essentials of care - emergent surgical debridement and broad antibiotic cover - and is most valuable when started early.
Pathophysiology
Gas gangrene is most often caused by Clostridium perfringens, a spore-forming anaerobe that flourishes in the low-redox environment of devitalised or contaminated tissue. Its alpha-toxin (a phospholipase C) and theta-toxin drive myonecrosis, vascular thrombosis and a spreading zone of ischaemia that outpaces the visible wound, with systemic toxaemia and haemolysis.
Why oxygen matters
Raising tissue oxygen tensions to the levels achievable at ~3 ATA is directly inhibitory to C. perfringens and, critically, suppresses alpha-toxin production. HBO also restores the oxygen-dependent oxidative killing of neutrophils and helps demarcate viable from non-viable tissue, which can reduce the extent of debridement required and limit progression while surgery and antibiotics take effect.
Role in management
- HBO never replaces surgery: aggressive, repeated debridement of necrotic tissue remains the priority.
- Antibiotics (commonly high-dose penicillin with clindamycin to suppress toxin synthesis) and full critical-care support are given concurrently.
- HBO is integrated early and does not delay theatre; the two are coordinated, not sequential.
Treatment approach
Typical protocols deliver HBO at pressures around 3 ATA, with several treatments in the first 24 hours and continued treatments over the following days, individualised to the surgical course and clinical response. Exact pressures, durations and frequency are set case by case at the unit.
Evidence base
Given the rarity and fulminant course of the condition, a randomised trial of HBO against no HBO is neither ethical nor feasible; the evidence is observational and experimental. The mechanistic rationale is strong: at hyperbaric pressure (2.8-3.0 ATA) tissue oxygen tension rises high enough to suppress clostridial alpha-toxin production and restore oxygen-dependent neutrophil bactericidal function.
Clinical cohorts are consistent in direction but mixed in significance: some (Hart 1983; Wilkinson & Doolette 2004) report lower mortality and less amputation with adjunctive HBO, while a two-hospital comparison (Brown 1994) found no significant difference. A Cochrane review (2015) identified only two small, very-low-quality randomised trials and no trial of HBO versus no HBO, so efficacy cannot be established from randomised data. Experimental work (Stevens 1993) shows HBO is ineffective on its own but significantly additive when given early alongside penicillin or metronidazole.
Bottom line: HBO is an early adjunct to urgent surgical debridement and antibiotics - never a substitute for, or a reason to delay, surgery, which is the primary and time-critical treatment. The evidence is observational and mechanistic, and best outcomes depend on treating early.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 04 — Clostridial Myonecrosis
UHMS Indications, Ch. 04 — Clostridial Myonecrosis Hyperbaric Medicine Practice, Ch. 17 — Gas Gangrene
Hyperbaric Medicine Practice, Ch. 17 — Gas Gangrene HBOT for Clostridial Myonecrosis (overview)
HBOT for Clostridial Myonecrosis (overview) HBOT for Gas Gangrene & Necrotising Fasciitis
HBOT for Gas Gangrene & Necrotising FasciitisKey references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Clostridial Myositis and Myonecrosis (Ch. 4).
- Weenink RP, Giannakopoulos GF, van Hulst RA. Clostridial myonecrosis (gas gangrene). Undersea Hyperb Med. 2025;52(2):203-9.
- Yang Z, Hu J, Qu Y, Sun F, Leng X, Li H, Zhan S. Interventions for treating gas gangrene. Cochrane Database Syst Rev. 2015;(12):CD010577.
- Hart GB, Lamb RC, Strauss MB. Gas gangrene. J Trauma. 1983;23(11):991-1000.
- Wilkinson D, Doolette D. Hyperbaric oxygen treatment and survival from necrotizing soft tissue infection. Arch Surg. 2004;139(12):1339-45.
- Brown DR, Davis NL, Lepawsky M, Cunningham J, Kortbeek J. A multicenter review of the treatment of major truncal necrotizing infections with and without hyperbaric oxygen therapy. Am J Surg. 1994;167(5):485-9.
- Stevens DL, Bryant AE, Adams K, Mader JT. Evaluation of therapy with hyperbaric oxygen for experimental infection with Clostridium perfringens. Clin Infect Dis. 1993;17(2):231-7.
- Hussain H, Fadel A, Garcia E, et al. Clostridial myonecrosis: a comprehensive review of toxin pathophysiology and management strategies. Microorganisms. 2024;12(7):1464.
The Killer That Smells Like Sugar: 5 Surprising Realities of Gas Gangrene
1. Introduction: the race against the invisible
In the world of infectious disease, most pathogens are slow-burners that give the immune system time to mount a defence. Clostridial myonecrosis - commonly known as gas gangrene - is the terrifying exception. This is not merely an infection; it is a "rapidly progressive, non-pyogenic, invasive" metabolic emergency. It represents a total breakdown of the host-pathogen truce, where the bacteria don't just inhabit the body, they dismantle it at a cellular level.
In this specific medical crisis, time is the only currency that matters. The stakes are staggering: a patient can go from the first flicker of symptoms to a moribund, multi-organ failure state in as little as 12 hours. It is a race where the finish line is often tissue death or systemic shock, and the window for a winning intervention is vanishingly small.
2. The "silent" scream: when pain outpaces visibility
There is a cruel paradox at the heart of gas gangrene's early stages. To the casual observer, a patient's limb might look entirely normal - perhaps a bit shiny or tense, but otherwise unremarkable. Yet the patient is often in a state of absolute agony. This is the "silent" scream of the deep tissue, where the pain is a direct result of rapid muscle destruction occurring far beneath the skin's surface.
For the clinician, this diagnostic paradox is the most vital warning sign. If the pain seems "wrong" for the visible injury, the alarm must be sounded immediately.
"Seemingly disproportionate pain in a clinically still-normal area must make the clinician highly suspicious for developing gas gangrene."
In the context of post-operative recovery or trauma, waiting for the skin to turn black is a death sentence. The pain is the primary signal that a metabolic "factory" has been established and is already churning out lethal toxins.
3. A sickly sweet scent and feathered X-rays
As the infection takes hold, it leaves behind a trail of highly specific, almost macabre physical signatures. These are not the typical signs of a pus-filled infection; gas gangrene is non-pyogenic, meaning the body is so overwhelmed it doesn't even produce pus. Instead, it produces the following:
- The sickly sweet odour: a thin, blood-tinged (serosanguinolent) fluid begins to seep from the area, carrying a distinctive, sickly sweet scent that experienced surgeons never forget.
- The "bruise" that won't stop spreading: the skin undergoes a rapid, terrifying transformation. It begins as shiny and tense, shifts to a dusky hue, and eventually settles into a deep bronze discolouration - a bruise that marks the death of the tissue beneath.
- Featherlike figures: on an X-ray, the image looks strangely delicate, almost like a bird's wing. These "featherlike figures" are actually gas bubbles - macabre metabolic byproducts - physically dissecting and separating the muscle fibres from one another.
- The surgical ghost: perhaps the most haunting sign occurs in the operating room. When a surgeon cuts into the affected muscle, there is a "biological silence." The muscle is a dark red, black, or greenish mass that does not bleed and has lost all ability to contract. It is dead tissue still trapped within a living body.
4. The toxin factory: why the body can't fight back
To understand why this disease is so lethal, one must look at the bacteria - primarily Clostridium perfringens - as a high-speed toxin factory. The primary weapon is alpha-toxin, a haemolytic agent that destroys platelets and white blood cells while causing widespread capillary damage. It is often paired with perfringolysin O (PFO), which works synergistically to cause direct vascular injury.
However, the "investigative" reality of this killer is that it doesn't always need an external wound to strike. Spontaneous (atraumatic) gas gangrene, often caused by C. septicum, can emerge from within. This specific bacterium is more aerotolerant and can seed itself into healthy muscle from the gut, often acting as a silent harbinger of hidden colonic or gynaecologic malignancies.
Once established, the "factory" effectively shuts down the body's defences through a process called vascular leucostasis. The toxins don't just block the delivery of white blood cells to the site; they actually inhibit neutrophil and erythroid differentiation in the bone marrow, essentially sabotaging the immune system's production line. The infection moves so fast that the patient often dies before their body can even begin to produce natural antitoxins.
5. Hyperbaric oxygen: stopping the toxin at the source
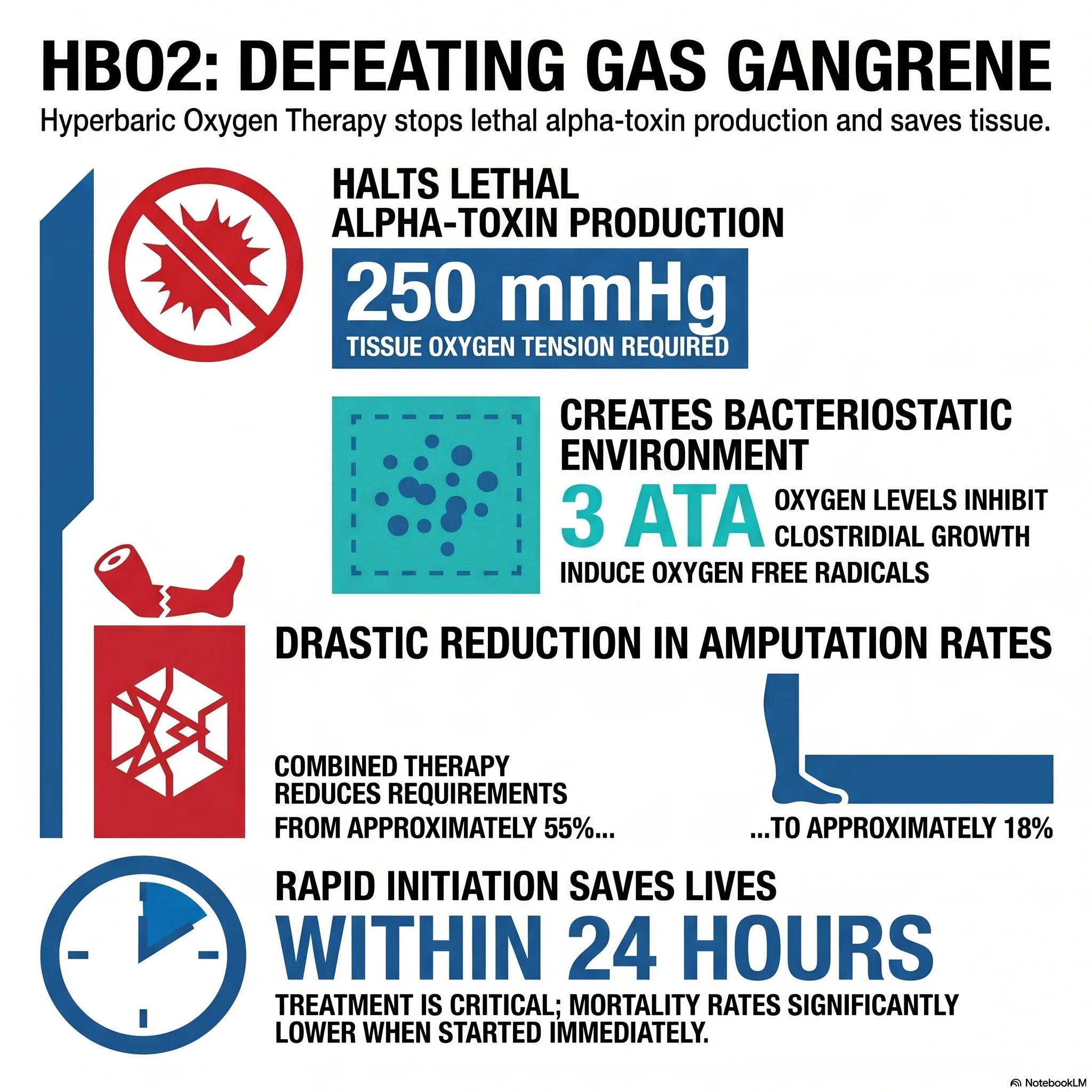
Standard antibiotics and surgery are often not enough because they cannot keep pace with the continuous production of alpha-toxin. This is where hyperbaric oxygen therapy (HBO2) becomes a critical, counter-intuitive tool. C. perfringens is not a strict anaerobe; it can actually survive in oxygen tensions up to 70 mmHg. To truly stop the toxin factory, you need an overwhelming force.
Research shows that an oxygen tension of 250 mmHg is required to halt alpha-toxin production entirely. By placing the patient in a hyperbaric chamber at 3 atmospheres absolute (3 ATA), clinicians can drive tissue oxygen levels above 300 mmHg, effectively "turning off" the bacteria's ability to kill.
HBO2 also serves as a vital "limb-saving" measure. By oxygenating still-viable tissue, it creates a clear "demarcation" between what is truly dead and what can be saved. This prevents surgeons from performing premature or overly aggressive amputations on patients who are already in shock. The effectiveness of this "triple therapy" (surgery, antibiotics, and HBO2) is starkly reflected in the data:
| Treatment group (dog model) | Survival rate |
|---|---|
| Surgery alone | 0% |
| Hyperbaric oxygen alone | 0% |
| Surgery + antibiotics | 70% |
| Triple therapy (surgery, antibiotics & HBO2) | 95% |
6. The gold standard paradox: when trials become unethical
In modern medicine, we demand randomised controlled trials (RCTs) as the "gold standard" of proof. Yet, for gas gangrene, there are no modern RCTs. This isn't a failure of science, but a victory of ethics.
Early observational studies showed such a massive improvement in survival with the addition of HBO2 that medical authorities reached a consensus: it would be morally indefensible to withhold oxygen from a control group just to prove what the data already showed.
"Because of these favorable results in observational studies, a randomized trial including a control group that does not receive HBO2 has been (and is) generally regarded as unethical."
Because of this, the European Committee for Hyperbaric Medicine gives HBO2 a Type 1 recommendation - the highest level of endorsement - acknowledging that when lives are measured in hours, clinical ethics and expert consensus must supersede the need for a "gold standard" trial.
7. Conclusion: a final thought on medical precision
Defeating gas gangrene requires a perfectly synchronised "triple therapy" counter-offensive. There is no room for delay. Success depends on a clinician's ability to trust their senses - to recognise that sickly sweet scent or that "disproportionate pain" - and to act before the lab results even return.
This disease forces us to confront the limits of traditional evidence-based medicine. It reminds us that in the face of a metabolic emergency, our most advanced technology is sometimes as simple as the air we breathe, concentrated and pressurised to overpower a microscopic killer. In the race against a toxin that outruns the immune system, the survival rates and the sheer biological weight of the evidence make concentrated oxygen one of our best hopes.
This feature article is general educational information and does not replace advice from your own doctor or emergency services. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.