Hyperbaric Oxygen Therapy for Refractory Osteomyelitis
When a bone infection keeps coming back despite proper surgery and antibiotics, hyperbaric oxygen can be added - raising the oxygen inside the infected bone to help the body and its treatment win.
What this means for you
What is refractory osteomyelitis?
Osteomyelitis is an infection of the bone. Most cases settle with antibiotics and, where needed, an operation to clean out the infected area. Sometimes, though, the infection keeps coming back or simply will not clear - this is called refractory or chronic osteomyelitis. Part of the reason is that infected bone often has a poor blood supply, so it receives too little oxygen and too little of the antibiotic.
How can hyperbaric oxygen help?
In the hyperbaric chamber you breathe pure oxygen under pressure, which raises the oxygen level inside the infected bone. Oxygen helps your body's infection-fighting cells do their job, improves the way some antibiotics work, and supports the healing of bone and surrounding tissue - especially after the infected area has been cleaned out surgically. It is used as an add-on in difficult cases, not on its own.
What to expect
When used, hyperbaric oxygen is given as a course of regular daily sessions over several weeks, alongside your surgery and antibiotic treatment. Whether it is suitable depends on the type and site of the infection and your overall health.
Is it safe?
Hyperbaric oxygen is generally well tolerated. The most common sensation is pressure on the ears during compression, much like descending in an aeroplane. Serious side effects are uncommon. You can read more on our risks and side effects page.
Watch
 The Stubborn Infection (English)
The Stubborn Infection (English) 'n Hardnekkige Infeksie (Afrikaans)
'n Hardnekkige Infeksie (Afrikaans) For Patients: Refractory Osteomyelitis (UHMS 12)
For Patients: Refractory Osteomyelitis (UHMS 12)This page is general health information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on your individual circumstances.
Clinical summary
Indication
Chronic refractory osteomyelitis - osteomyelitis that persists or recurs after appropriate surgical and antibiotic therapy - is a recognised indication for adjunctive hyperbaric oxygen (HBO) therapy under the Undersea & Hyperbaric Medical Society (UHMS). HBO is most relevant in compromised hosts and complex anatomy (e.g. Cierny-Mader physiologic class B), and never substitutes for source control.
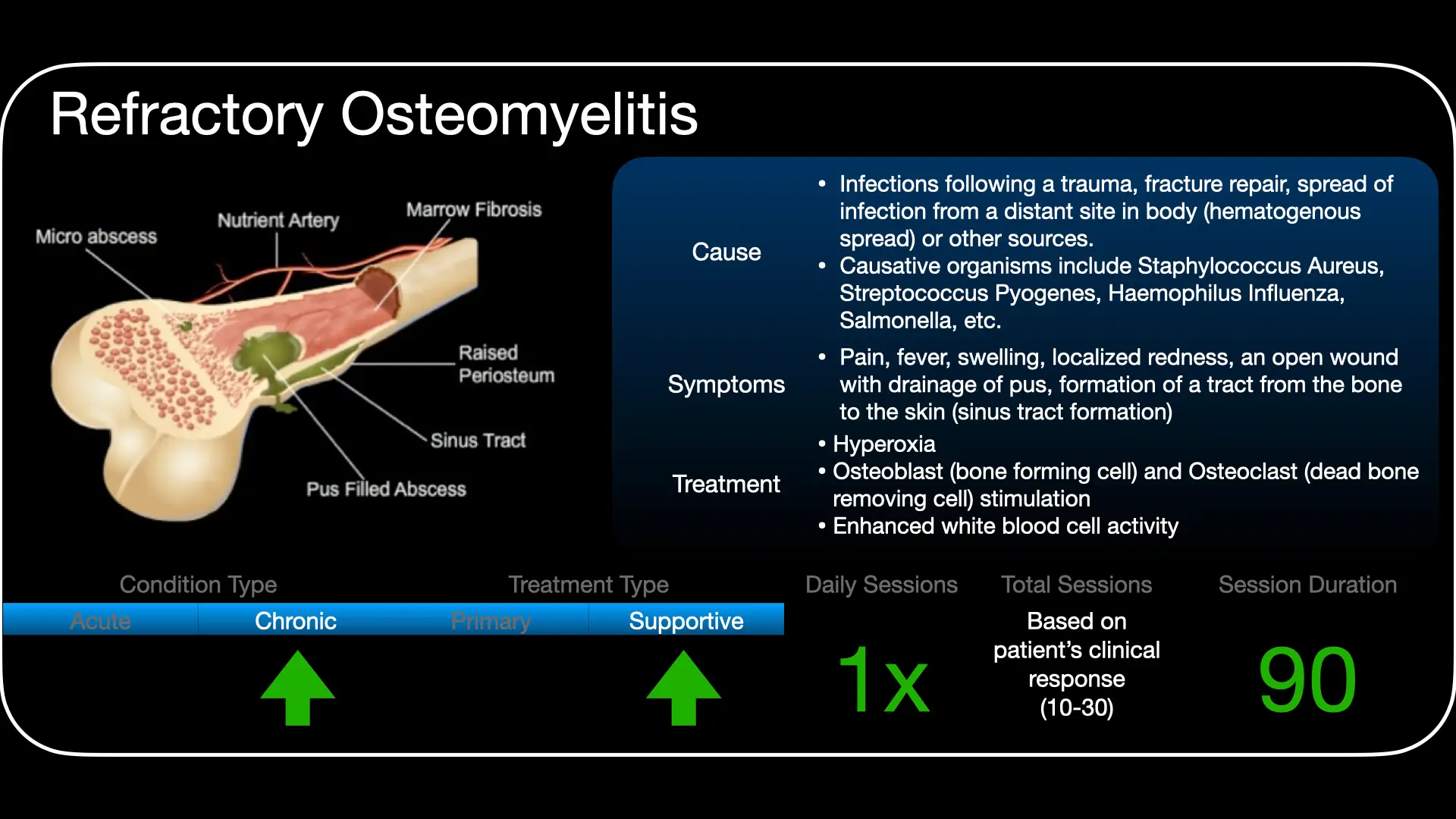
Pathophysiology
Chronic osteomyelitis is characterised by ischaemic, necrotic bone (sequestra), biofilm, and impaired host defence in a hypoxic microenvironment. Measured oxygen tensions in infected bone are low - well below those required for effective leukocyte oxidative killing - which helps explain persistence despite conventional therapy.
Why oxygen matters
HBO raises bone and soft-tissue oxygen tensions into the range needed to restore oxygen-dependent neutrophil bactericidal activity, enhances the activity and transport of certain antibiotics (notably aminoglycosides and fluoroquinolones are oxygen-dependent), is directly inhibitory to some anaerobes, and supports osteogenesis, angiogenesis and wound healing. The effect is synergistic with surgery and antibiotics.
Role in management
- Source control is essential: thorough debridement/sequestrectomy, dead-space management and culture-directed antibiotics come first.
- HBO is added in refractory or high-risk cases (compromised host, multiply-operated, marginal perfusion) to improve the chance of cure.
- Coordinate with orthopaedic/plastic surgery and infectious diseases; address vascular inflow where relevant.
Treatment approach
When indicated, HBO is delivered on 100% oxygen at pressures commonly around 2.0-2.4 ATA, daily, over a course typically in the order of 20-40 sessions (sometimes more), coordinated with surgery and the antibiotic course. Exact protocol is individualised and set case by case at the unit.
Evidence base
Randomised trials of HBO in osteomyelitis do not exist, so the evidence is observational - mechanism plus systematic reviews of clinical series. Two systematic reviews report high success when HBO is added to surgical debridement and culture-targeted antibiotics in refractory disease: Savvidou 2018 (460 patients across 45 studies; 73.5% successful outcome with no reported relapse) and Goldman 2009 (remission of about 85% of refractory lower-extremity osteomyelitis). A recent single-institution cohort (Jackson 2025) found that patients who completed the HBO course had nearly eight times the odds of improvement compared with those who did not complete it.
These success rates come from uncontrolled, selected series (all patients had already failed standard therapy), so the benefit is a consistent observational signal rather than proof. HBO restores the low oxygen tension of chronically infected bone - re-enabling neutrophil bacterial killing and the activity of oxygen-dependent antibiotics - with the strongest reported responses in mandibular and post-radiation osteomyelitis. Where surgery is not feasible (some deep vertebral, cranial or sternal cases), a trial of antibiotics with HBO may be considered.
Bottom line: HBO is an adjunct to surgical debridement and culture-targeted antibiotics for bone infection that has failed standard treatment. The observational evidence consistently associates it with higher cure rates, but this is an association, not proof - surgery and antibiotics remain the foundation. The course is long, typically 20-40 daily sessions.
Talks & chapter reviews
Recorded talks and textbook-chapter reviews on this indication:
 UHMS Indications, Ch. 12 — Refractory Osteomyelitis
UHMS Indications, Ch. 12 — Refractory Osteomyelitis HMP, Ch. 20 — HBO for Chronic Refractory Osteomyelitis
HMP, Ch. 20 — HBO for Chronic Refractory Osteomyelitis HBOT for Refractory Osteomyelitis (overview)
HBOT for Refractory Osteomyelitis (overview) HBOT for Osteomyelitis (overview)
HBOT for Osteomyelitis (overview)Key references
- Undersea & Hyperbaric Medical Society. Hyperbaric Oxygen Therapy Indications, 15th ed (2023) - Refractory Osteomyelitis (Ch. 12).
- Hart BB. Hyperbaric oxygen for refractory osteomyelitis. Undersea Hyperb Med. 2021;48(3):297-321.
- Savvidou OD, Kaspiris A, Bolia IK, et al. Effectiveness of hyperbaric oxygen therapy for the management of chronic osteomyelitis: a systematic review. Orthopedics. 2018;41(4):193-199.
- Goldman RJ. Hyperbaric oxygen therapy for wound healing and limb salvage: a systematic review. PM&R. 2009;1(5):471-479.
- Jackson JB 3rd, Bakaes Y, Jacques B, et al. Adjunctive hyperbaric oxygen therapy for patients with chronic refractory osteomyelitis: a report of treatment outcomes and risk factors for treatment failure. Adv Skin Wound Care. 2025;38(1):40-45.
- Memar MY, Yekani M, Alizadeh N, Baghi HB. Hyperbaric oxygen therapy: antimicrobial mechanisms and clinical application for infections. Biomed Pharmacother. 2019;109:440-447.
- Cierny G 3rd, Mader JT, Penninck JJ. A clinical staging system for adult osteomyelitis. Clin Orthop Relat Res. 2003;(414):7-24.
How Oxygen is Curing "Un-curable" Bone Infections
1. Introduction: the infection that won't quit
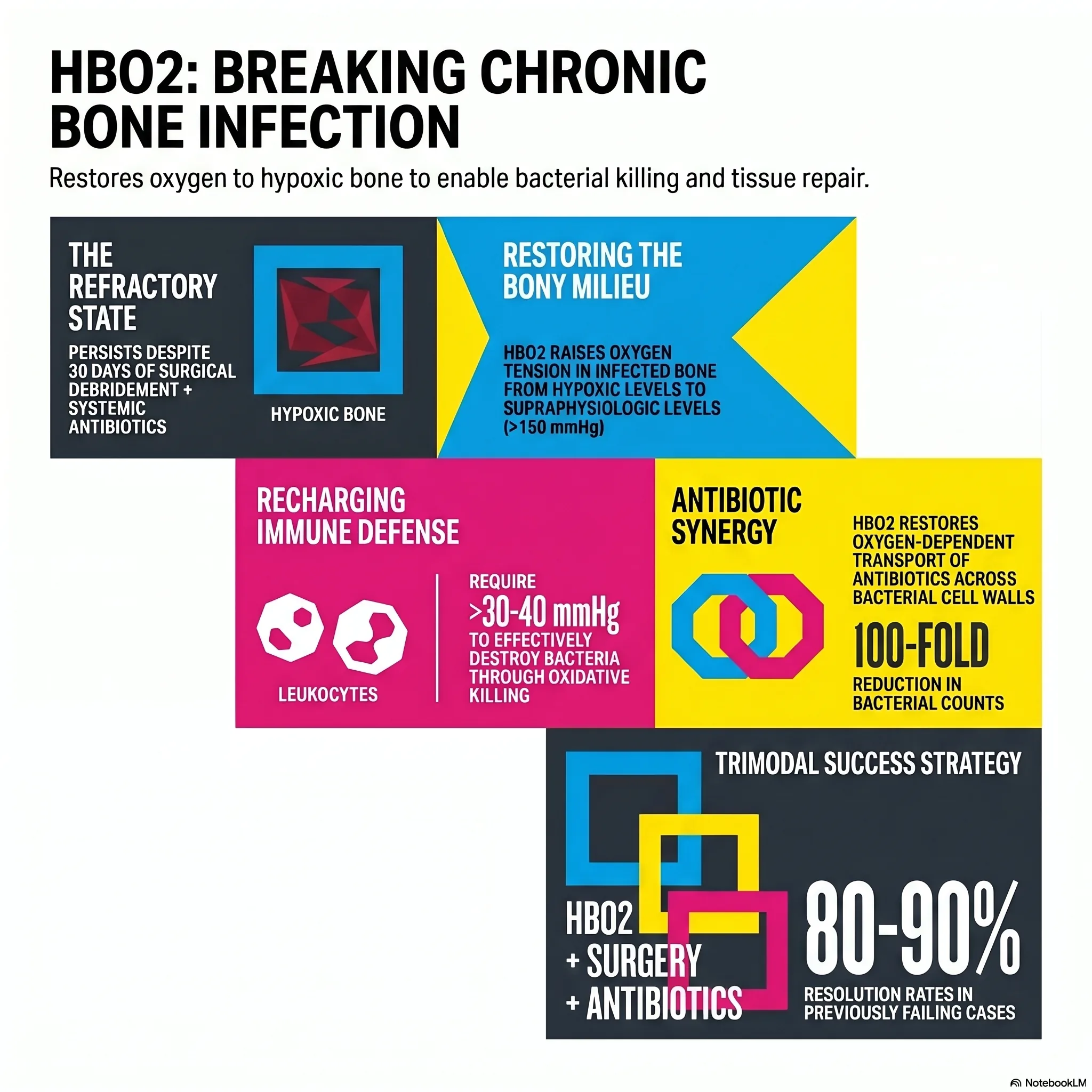
Chronic refractory osteomyelitis is the ultimate "medical stalemate." It is a gruelling cycle where bone - the very foundation of the body - becomes a fortress for bacteria. Patients often endure "sinus tracts" (painful, draining wounds) and the development of "sequestra" (segments of dead bone that have detached from their blood supply). When a case is deemed refractory - showing no significant improvement after 30 days of aggressive surgery and systemic antibiotics - the patient is often left with a grim prognosis: indefinite medication, radical disfigurement, or amputation.
The frustration for clinicians is that the failure isn't always the medicine; it is the environment. In the dark, oxygen-starved pockets of infected bone, standard treatments simply lose their power. Hyperbaric oxygen (HBO2) therapy is the innovation breaking this deadlock, not by replacing the current "gold standard", but by acting as the physiologic catalyst that allows the body to finally finish the fight.
2. The "force multiplier": the 100-fold antibiotic boost
One of the most profound breakthroughs in hyperbaric medicine is the discovery that oxygen is a transport mechanism for antibiotics. High-potency drugs like aminoglycosides (gentamicin, tobramycin) and cephalosporins require an oxygen-dependent electron transport system to cross bacterial cell walls. If tissue oxygen levels fall below 20-30 mmHg, this active transport is diminished - the medicine literally cannot get inside the bacteria to do its job.
By flooding the bone with oxygen at 2.4 to 2.5 atmospheres (ATA), HBO2 restores this transport mechanism, essentially "weaponising" antibiotics that were previously ineffective.
"The combination of cefazolin and HBO2 therapy produced a 100-fold greater reduction in bacterial counts than either antibiotics or HBO2 therapy alone."
3. Weaponising white blood cells: the "oxidative burst"
The body's primary defence against Staphylococcus aureus - the leading cause of bone infection - is the leukocyte (white blood cell). To kill bacteria, these cells perform an "oxidative burst", a chemical explosion that requires high levels of fuel. In infected bone, oxygen levels often plummet to a "hypoxic milieu" of 23 mmHg, leaving leukocytes paralysed and unable to defend the host.
Using the Mader et al. rabbit model, researchers demonstrated that leukocyte-mediated killing is significantly impaired in these low-oxygen environments but is fully restored - and even enhanced - when oxygen tensions are raised to physiologic or supraphysiologic levels.
Critical oxygen tension benchmarks:
- Infected bone (breathing air): ~23 mmHg - immune function impaired.
- Minimum threshold for killing: 30-40 mmHg - the survival line for immune defence.
- Normal bone (breathing air): ~45 mmHg - the baseline.
- Infected bone (HBO2 at 2 ATA): ~104 mmHg - immune function restored.
- Peak efficiency: 150 mmHg - optimal performance for bacterial eradication.
4. Avoiding the scalpel: saving the spine and skull
The standard treatment for osteomyelitis is often "radical debridement" - the surgical removal of infected bone. However, in sensitive areas like the cranium, spine, or sternum, the "scalpel first" approach carries extreme risks of morbidity or mortality. In these high-stakes scenarios, HBO2 offers a "reasonable prospect for cure" while leaving the bone and surgical hardware intact.
The shift here is profound: HBO2 is now an AHA Class IIa intervention for these sites, meaning the weight of evidence supports its use to avoid debilitating surgeries.
Priority sites for HBO2 intervention:
- The spine (AHA Class IIa): resolves iatrogenic infections without the need to remove stability-providing hardware or instrumentation.
- The cranium (AHA Class IIa): achieves nonsurgical cure rates of 70-100%, often saving devascularised bone flaps and prosthetics.
- The sternum (AHA Class IIa): drastically reduces mortality and helps avoid the 20-35% mortality rate associated with aggressive post-cardiac surgery debridement.
- Paediatrics (AHA Class IIa): protects the epiphysis (growth plate), preventing the lifelong disfigurement and growth arrest caused by radical bone removal in children.
5. The "B-host" advantage: levelling the playing field
Clinicians use the Cierny-Mader classification to judge how well a patient can fight an infection. While "A-hosts" have normal physiology, "B-hosts" suffer from systemic or local compromises that make healing nearly impossible. HBO2 acts as the ultimate physiological "equaliser", essentially shifting a B-host's healing potential toward that of an A-host.
Notably, for diabetic foot ulcers (Wagner Grade 3 or 4) with underlying osteomyelitis, HBO2 has earned the highest possible endorsement: AHA Class I.
Compromising factors for "B-hosts":
- Systemic (Bs): diabetes mellitus, tobacco use, malnutrition, renal failure, malignancy, and extremes of age.
- Local (BL): chronic lymphoedema, venous stasis, major vessel compromise, radiation fibrosis, and extensive scarring.
6. The ROI of oxygen: why high-tech is actually cheaper
While a course of 20 to 40 HBO2 sessions represents a significant upfront cost, it is a rounding error compared to the "tail" of expense for a failed cure. When standard treatments fail, the costs of repeat surgeries, long-term ICU stays, and disability are astronomical.
Data from the Larsson study shows that primary cures achieved with HBO2 in cranial cases confer a 48-66% saving over the cost of repeat craniotomies. Furthermore, research by Yu et al. (2011) showed that in sternal infections, adjunctive HBO2 slashed ICU stays from an average of 48.8 days to just 8.7 days.
"Cost-effectiveness was calculated as being five-fold in favour of adjunctive HBO2 therapy in refractory osteomyelitis."
7. Conclusion: a new horizon for bone health
Hyperbaric oxygen therapy has moved beyond the realm of the experimental. While we await "conclusive randomised clinical trials", the accumulated weight of 44 authoritative studies (animal and human) has established HBO2 as a clinical necessity. It is the vital third leg of the "management triad": surgery + antibiotics + oxygen.
"A trial of systemic culture-directed antibiotics and HBO2 therapy prior to undertaking more than limited surgical interventions provides a reasonable prospect for osteomyelitis cure."
A final thought: in the world of innovation, we often look for new molecules or complex robotics. But here, the breakthrough is a fundamental element. When delivered at 2.4 atmospheres, we must stop viewing oxygen as merely a gas we breathe - it is a powerful, evidence-backed drug that can heal what was once considered un-curable.
This feature article is general educational information and does not replace advice from your own doctor. Whether hyperbaric oxygen is appropriate depends on individual circumstances. Portions were drafted with the assistance of AI tools and reviewed by Dr Gregory Weir; please verify clinical details against primary sources.
Speak to the unit
The Vascular & Hyperbaric Unit, Life Eugene Marais Hospital, Pretoria.
Call 012 335 8651► Browse all Educational Hyperbaric Oxygen Therapy Videos
Medically reviewed by Dr Gregory Weir, vascular surgeon. Last updated July 2026.